Real-world outcomes of oral anticoagulation in atrial fibrillation patients with high bleeding and stroke risks: evidence from three international registries from Middle East, Europe and Asia-Pacific
European Heart Journal


Abstract
The use of oral anticoagulants (OACs) in patients with atrial fibrillation (AF) for stroke prevention should be balanced between the reduction on stroke risk and the increase in bleeding.
This study aimed to evaluate the outcomes of atrial fibrillation (AF) patients at high risk of both bleeding (HAS-BLED score ≥3) and stroke (CHA₂DS₂-VASc score ≥2). The primary objective was to identify factors associated with the composite outcome of all-cause mortality, acute coronary syndrome (ACS), major adverse cardiovascular events (MACE), and thromboembolic events. Secondary objectives included determining significant predictors of individual outcomes such as all-cause mortality, ACS, MACE, major bleeding, OAC therapy and thromboembolic events in this high-risk population.
We analyzed data from three AF patient registries: EORP-AF, APHRS, and IRAF (Table 1). Patients included in the study had a CHA₂DS₂-VASc score of ≥2 and HAS-BLED score ≥3. Baseline characteristics were compared using the Chi-Square or Fisher’s Exact Test for categorical variables and the T-Test or Wilcoxon Test for continuous variables. Multivariable logistic regression was performed to identify significant predictors of OAC use, as well as key clinical outcomes, including the composite outcome of all-cause mortality, ACS, MACE, and thromboembolic events. Statistical analyses were conducted using R (version 4.3.1).
A total of 2,535 patients (58.3% male, mean age 75.39±7.82 years) were analyzed, with 80.3% (n=2,037) receiving OAC therapy.
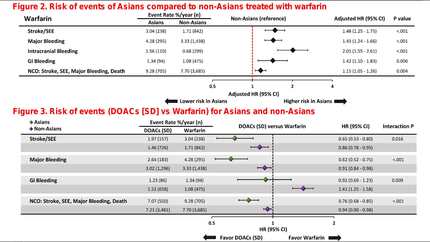
Female patients had a 43% lower likelihood of experiencing major bleeding within one year compared to male patients (OR=0.573, 95% CI: 0.331–0.964, P=0.040). A prior history of major bleeding was a strong predictor of future bleeding events, with a more than threefold increased risk (OR=3.143, 95% CI: 1.872–5.228, P<0.001). Additionally, patients of Asian ethnicity had significantly lower odds of developing major bleeding within one year (OR=0.281, 95% CI: 0.105–0.626, P=0.005). Patients with a BMI <18 had significantly higher odds of experiencing thromboembolic events within one year (OR=5.801, 95% CI: 0.845–24.289, P=0.031) (figure 1). Asian ethnicity was associated with a 58% lower risk of the composite outcome compared to European ethnicity (OR=0.422, 95% CI: 0.274–0.633, p<0.001).
In AF patients with high risk of bleeding and stroke, OAC therapy was associated with a significantly lower risk of the composite outcome including all-cause mortality, ACS, MACE, and thromboembolic events at 1 year follow-up. Given the significant impact of factors such as age, comorbidities, and ethnicity on outcomes, tailored treatment approaches should be considered in clinical decision-making. Baseline characteristics Forest plots
Contributors

A Askarinejad
Author
Institute of Life Course and Medical Sciences Liverpool , United Kingdom of Great Britain & Northern Ireland

T Bucci
Author

S H M Lam
Author
University of Liverpool Liverpool , United Kingdom of Great Britain & Northern Ireland
E Tartaglia
Author
M Rossi
Author
M Zhao
Author
H Tse
Author




G Y H Lip
Author
University of Liverpool Liverpool , United Kingdom of Great Britain & Northern Ireland
You may be interested in