Inhibition of the programmed death protein 1 immune checkpoint and the development of heart failure in the presence of prior cardiac ischaemia
Cardiovascular Research


Abstract
Immune checkpoint inhibitors (ICIs) have revolutionized cancer treatment. However, their use often leads to cardiovascular adverse effects, including cardiac dysfunction. Here, we hypothesized that a prior cardiac ischaemic injury could exacerbate cardiac dysfunction due to anti-programmed death protein 1 (PD-1) treatment. Furthermore, we investigated whether abatacept, a T-cell costimulation blocker, could ameliorate the ICI-induced cardiotoxicity in a pre-clinical model.
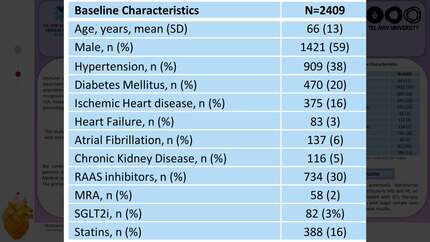
In a pre-clinical study, mice were treated with isoprenaline or control to induce reversible cardiac ischaemia. After 16 weeks of follow-up, recovery of cardiac function was confirmed via echocardiography, and mice from both groups were randomly treated with isotype control, anti-PD-1, or anti-PD-1 combined with abatacept, for 2 further weeks. Mice with prior ischaemic injury and anti-PD-1 treatment showed cardiac dysfunction with increased infiltration of T cells and macrophages and elevated expression of pro-inflammatory cytokines. Conversely, cardiac dysfunction and inflammation were less pronounced after anti-PD-1 treatment in mice without prior ischaemic injury. Mice with concomitant abatacept treatment exhibited normal cardiac function and alleviated pro-inflammatory response. In a parallel single-centre retrospective clinical cohort study, 1671 cancer patients receiving PD-1 inhibitors were analysed. Cases were defined as patients who developed incident heart failure (HF) after ICI initiation with a primary aim to test whether pre-existing ischaemic heart disease was associated with an increased risk for HF development post-ICI therapy. Sensitivity analyses included propensity score matching and comparison with non-ICI-treated cancer patients. Among ICI-treated patients, 109 (6.5%) developed HF over a median follow-up of 332 days. Multivariable logistic regression of the matched population showed increased odds of incident HF in patients with prior ischaemic cardiac events (odds ratio 2.11, 95% confidence interval 1.05–4.2,
In mice, induction of cardiac inflammation and dysfunction by anti-PD-1 therapy was potentiated by prior transient ischaemic cardiac injury, which was ameliorated by abatacept cotreatment. Cancer patients with pre-existing ischaemic heart disease may be at greater risk for developing ICI-induced new-onset HF. Based on our findings, cardiac surveillance should be considered in patients starting ICI therapy with a prior history of ischaemic heart disease.
Contributors

Tamás G Gergely
Author
Zsófia D Drobni
Author
Tamás Kovács
Author
Nabil V Sayour
Author
Viktória E Tóth
Author
Márton S Kocsis
Author
Zsófia Onódi
Author
Gábor M Mórotz
Author
Andrea Kovács
Author
Daniel A Zlotoff
Author
Hannah K Gilman
Author
Jingyi Gong
Author
Nóra Fekete
Author
Éva Pállinger
Author
Edit I Buzás
Author
Laura I Yousif
Author
Wouter C Meijers
Author
Béla Merkely
Author
Kerry L Reynolds
Author
Péter Ferdinandy
Author
Tomas G Neilan
Author

You may be interested in