Uprising heart failure therapies for cardio-permissive strategies in cancer therapy-related cardiac dysfunction
European Heart Journal Supplements


Abstract
Permissive cardiotoxicity is a novel concept in cardio-oncology that balances the need for life saving oncological therapy with the acceptance of its cardiotoxicity. One of the most feared cardiotoxicities of chemotherapy (QT) is cancer therapy-related cardiac dysfunction (CTRCD) which often leads to premature QT discontinuation. Change in left ventricular ejection fraction (LVEF) and global longitudinal strain (GLS) define the CTRCD according to 2022 ESC Cardio-oncology guidelines.
Retrospective analysis of outpatients (P) diagnosed with CTRCD, followed at a cardio-oncology clinic at a tertiary centre between April 2021 and December 2023, managed with a permissive cardiotoxicity strategy without subsequent QT discontinuation.
20P were included with a mean age of 56±12 years, 80% were women. Most common malignancies were breast cancer (65%) and hematologic neoplasms (25%); 45% were stage IV. The major of cardiotoxic QT were HER2-targets (55%) and anthracyclines (15%). There was a high burden of CV risk factors (≥2 in 55%). The median follow-up was 16 months (IQR 11-27).
Most patients (85%) presented mild or moderate asymptomatic CTRCD. The cohort presented a median baseline of LVEF 61% (IQR 58-65) and GLS -17.5% (-15.2 to -18.2%). Both presented a significant decrease during QT to a median minimum LVEF of 49% (p<0.001) and GLS -13.9% (p=0.028). An increase in NT-proBNP levels (median 2x increase) was observed in 9 (45%), with a median maximum of 1805 pg/mL. Only 3P experienced mild-to-moderate symptomatic HF due to toxicity, 1 requiring hospitalization.
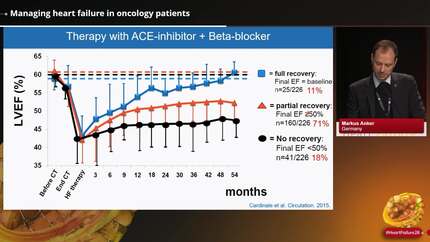
All patients received cardioprotective therapy (95% under ≥2 HF pillar classes; 25% under sacubitril-valsartan). With permissive strategy, 13P (65%) completed the entire oncological treatment, with a post-treatment median LVEF of 57% (53–61) and GLS of -15.2% (-15.5-18.2%), showing no significant difference compared to baseline (p>0.05). 7P remain on QT, 6 of whom are under palliative treatment despite cardiac dysfunction for over 12 months (range: 14 to 36 months). No mortality or severe cardiovascular-related adverse events were reported.
A permissive cardiotoxicity strategy supported by optimized cardiac care and close monitoring allowed patients with mild-to-moderate CTRCD to safely maintain QT with cardioprotective therapy. These findings underscore the importance of structured cardio-oncology follow-up in enabling high-risk patients to complete oncological therapies. Supplementary data
Contributors

R Carvalheiro
Author
I Cardoso
Author
V Vaz Ferreira
Author
T Branco Mano
Author
L Almeida Morais
Author
R Cruz Ferreira
Author
You may be interested in