The COR Lipid-Registry: The effectiveness of the strike early and strike strong strategy (SES) in patients with high cardiovascular risk
European Heart Journal - Acute CardioVascular Care


Abstract
According to real world data only up to 20 % of patients with atherosclerotic cardiovascular disease (ASCVD) are below the recommended LDL-cholesterol (LDL-C) target of < 55mg/dl (<1.4 mmol/L) 1-3 months after the index event. Accordingly, improved strategies for initiating lipid-lowering therapy (LLT) are desired to achieve treatment targets required to further reduce future cardiovascular event rates.
The COR Lipid Registry included patients at very-high cardiovascular (CV) risk presenting for percutaneous coronary intervention (PCI) with acute (ACS) or chronic (CCS) coronary syndrome. Coronary artery disease (CAD) patients with an LDL-C level of >130 mg/dL (equalizing 3.37 mmol/L), or a non-HDL of 160mg/dL (equalizing 4.14 mmol/L) either LLT-naïve or with suboptimal LLT at index hospitalization were enrolled. Based on lipid levels at baseline, these patients were assumed to need triple LLT to achieve their LDL-C target. Baseline characteristics and lipid parameters of all patients were collected at index hospitalization and 2 follow-up visits, after 4-6 and 8-12 weeks, respectively. Initially, in all patients a dual LLT (high-dose, highly effective statin, which means atorvastatin 40mg or 80mg and rosuvastatin 20mg or 40mg, plus ezetimibe) was initiated during the index hospitalization, before PCSK9-inhibitors or bempedoic acid were added, if LDL-C target levels were not met at control visits.
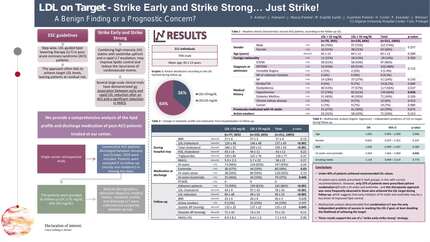
In total, 165 very-high-risk patients were included, of which 79 (42.0%) were admitted for CCS, and 109 (58%) for ACS, respectively. At visit 1, 114 (69.1%) patients reached the recommended (ESC/EAS guidelines 2019) lipid goals (LDL-C of < 55 mg/dl; equalising 1.4 mmol/L; or non-HDL-C of 85 mg/dl equalizing 2.2 mmol/<l), (n="64),">
Summary: An optimized LLT-strategy for managing a very-high CV risk patient cohort undergoing PCI, starting with a dual LLT-strategy consisting of a high-dose, highly effective statin plus ezetimibe at the index event followed by addition of a third LL-agent (a PCSK9-inhibitor or bempedoic acid) at follow-up after 4-6 weeks if treatment goal was not reached, was highly effective in achieving LDL-C and non-HDL-C goals. Wider adoption of this strategy may help to significantly improve LDL-C-target levels in real-world populations in very-high risk CAD patients presenting with ACS or CCS for coronary revascularisation.</l),>
Contributors



You may be interested in