Complete revascularization timing in ST-segment elevation myocardial infarction and multivessel disease with heart failure: the OPTION–STEMI trial
European Heart Journal


Abstract
The optimal timing of complete revascularization in patients with ST-segment elevation myocardial infarction (STEMI) and multivessel disease complicated by heart failure remains uncertain.
The OPTION-STEMI (Optimal Timing of Fractional Flow Reserve-Guided Complete Revascularization for Non-Infarct-Related Artery in ST-segment Elevation Myocardial Infarction with Multivessel Disease) trial compared immediate vs staged complete revascularization during the index admission in patients with STEMI and multivessel disease. In the OPTION-STEMI trial, immediate complete revascularization was not found to be non-inferior for the primary endpoint compared with staged complete revascularization. Pre-specified subgroup analysis was performed according to heart failure at admission, defined as Killip class II or III. The primary endpoint was a composite of death from any cause, non-fatal myocardial infarction, or any unplanned revascularization at 1 year.
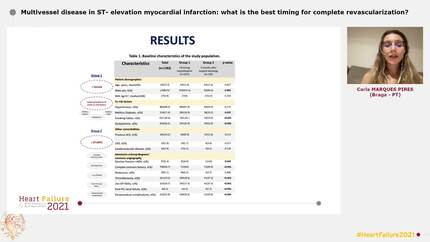
Among 994 randomized patients, 329 (33.1%) had heart failure at admission. These patients had a higher risk of primary endpoint than those without heart failure (18.2% vs 8.7%; adjusted HR 1.63; 95% CI 1.11–2.40;
In the OPTION-STEMI trial, among patients with STEMI and multi-vessel disease who were not in cardiogenic shock, immediate complete revascularization was not non-inferior compared with staged complete revascularization. However, subgroup analysis suggests that the worse outcomes with immediate complete revascularization may be limited to patients with heart failure at admission. Further studies are required to demonstrate the non-inferiority of immediate complete revascularization compared with staged complete revascularization in patients without heart failure.
Contributors

Min Chul Kim
Author
Joon Ho Ahn
Author
Dae Young Hyun
Author
Yongwhan Lim
Author
Kyung Hoon Cho
Author

Seongho Park
Author
Seok Oh
Author
Doo Sun Sim
Author
Young Joon Hong
Author
Ju Han Kim
Author
Myung Ho Jeong
Author
Jang Hyun Cho
Author
Sang-Rok Lee
Author

Jin-Yong Hwang
Author

Jung-Hee Lee
Author
Jong-Hwa Ahn
Author
Dong-Bin Kim
Author
Eun Ho Choo
Author
Chan Joon Kim
Author
Weon Kim
Author
Jay Young Rhew
Author
Jong-Il Park
Author
Sang-Yong Yoo
Author

You may be interested in