Sex differences in recurrence after atrial fibrillation ablation in patients with low-voltage areas: results from the SUPPRESS-AF trial
European Heart Journal


Abstract
Female sex is a known risk factor for the presence of low-voltage areas (LVAs) and post-ablation recurrence in patients with atrial fibrillation (AF).
This study aimed to evaluate sex differences in AF recurrence after pulmonary vein isolation (PVI-alone) versus PVI plus LVA ablation (PVI+LVA-ABL).
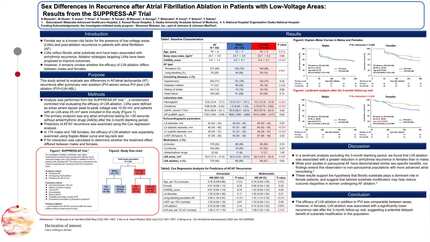
An analysis was performed from the SUPPRESS-AF trial, a randomized controlled trial evaluating the efficacy of LVA ablation. LVAs were defined as areas where bipolar peak-to-peak voltage was <0.50 mV, and patients with an LVA area ≥5 cm² were included in this study. The primary endpoint was any atrial arrhythmia lasting for >30 seconds without antiarrhythmic drugs (AADs). Arrhythmia episodes identified during the 3-month blanking period are not considered AF recurrences.
Among 339 study patients, 165 (48.7%) were females. Females were older than males (76 [IQR, 69–78] vs. 74 years [IQR, 72–79], p=0.014) and had larger LVA areas (16.4 cm² [IQR, 10.0–28.6] vs. 11.7 cm² [IQR, 8.1–19.7], p<0.001). At one year post-ablation, recurrence rates were similar between the PVI-alone and PVI+LVA-ABL groups in males (42.5% vs. 42.4%, log-rank p=0.92). In females, the PVI+LVA-ABL group exhibited a trend toward lower recurrence compared to the PVI-alone group (42.7% vs. 30.1%, log-rank p=0.10, P for interaction=0.17).
Excluding patients with persistent AF recurrence or AAD use at 3 month, a landmark analysis beyond the blanking period demonstrated that the recurrence rates remained compatible in males (33.3% vs. 32.4%, log-rank p=0.91). However, in females, the recurrence rate was significantly lower in the PVI+LVA-ABL group compared to the PVI-alone group (43.8% vs. 23.3%, log-rank p=0.013), with a P for interaction of 0.080.
The efficacy of LVA ablation in addition to PVI was compatible between sexes. However, in females, LVA ablation was associated with a significantly lower recurrence rate beyond the blanking period, suggesting its potential efficacy as a substrate modification strategy in female patients.





You may be interested in