Hypokalemia as a trigger for atrial fibrillation: Insights from patients with implantable loop recorders
European Heart Journal


Abstract
Low potassium is considered an important risk factor for atrial fibrillation (AF), but recent studies have failed to demonstrate decreased AF occurrence with potassium supplementation.
To investigate potassium imbalance as a trigger for AF in patients undergoing long-term continuous monitoring.
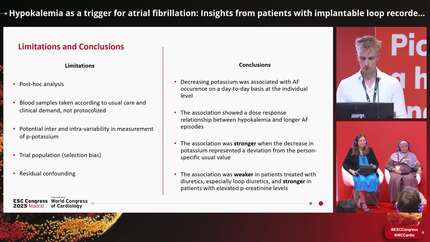
Post-hoc analysis of the LOOP study randomising AF-naïve participants with risk factors for AF and stroke to long-term implantable loop recorder (ILR) monitoring vs usual care. AF episodes lasting at least 6 minutes were adjudicated by cardiologists. This study analysed the ILR data according to all blood samples collected as part of the trial or routine clinical practice (general practice, outpatient clinic, hospitalization) within 1 day from each day of monitoring. Logistic regression was applied to assess the association between plasma potassium concentration and AF occurrence unadjusted, adjusted for sex, age, and comorbidities (hypertension, diabetes, thyrotoxicosis, valvular disease, heart failure, and previous acute myocardial infarction), and adjusted for AF burden during all of monitoring. A threshold of minimum 1 hour of AF was applied in the main analysis, while additional analyses were grouped by daily AF duration <1, 1-2, 2-4, and >4 hours. Hypokalemia was defined as p-potassium<3,5 mmol/L.
A total of 1333 participants with available ILR raw data and blood samples were included (89% of all randomised to ILR), mean age 75±4.1 years, 46% women, 92% with hypertension, and 29% diabetes. The combined dataset included more than 1.6 million days of continuous monitoring, of which 50,746 were with adjudicated AF, and 12,136 measurements of p-potassium taken during continuous monitoring.
Potassium was lower in measurements within 1 day from AF detection compared to without AF (mean 3.91 vs 3.99 mmol/L; difference -0.08 (95% CI: -0.12 to -0.05; p <.0001), Figure 1). Using a nonlinear mixed-effects model yielded a difference of -0.21 mmol/L (95% CI: -0.25 to -0.18; p <.0001).
In unadjusted models, the odds of AF occurrence increased with 33% for every unit decrease in potassium (OR 0.67 (95% CI (0.56-0.79)), which was robust to adjustment for sex, age, and comorbidities (OR 0.63 (95% CI (0.53-0.75)), and AF burden (OR 0.56 (95% CI (0.46 – 0.69)). When AF occurrence was grouped by daily AF duration, a dose-response pattern emerged with 5.1% of AF episodes lasting below 1 hour coinciding with hypokalemia increasing to 19.1% for AF episodes lasting above 4 hours (Figure 2).
In patients with risk factors for AF and stroke undergoing continuous monitoring, we found an association between decreased potassium and AF occurrence, with dose-response relation indicating higher impact of hypokalemia on longer AF episodes. These findings are explorative, and further studies are needed to distinguish patterns of potassium imbalances and the effect on AF in different patient groups.





You may be interested in