Cardiac rehabilitation improves subclinical left ventricular dysfunction in patients after cardiac surgery
European Journal of Preventive Cardiology


Abstract
Left ventricular global longitudinal strain (GLS) provides analysis of global systolic function and quantifies myocardial deformation. In presence of preserved left ventricular ejection fraction, GLS allows to detect subclinical dysfunction in different clinical scenarios. New studies on the use of this tool in the field of cardiac rehabilitation are growing. However, these investigations are showing conflicting data on the improvement in GLS due to the training exercise. Further research is needed to define the role of left ventricular GLS and impact of cardiac rehabilitation program.
The aim of our study was to assess the impact of cardiac rehabilitation program on GLS in patients with preserved left ventricular ejection fraction and after cardiac surgery. Furthermore, an optimal baseline cut-off value to predict the improvement in GLS after the rehabilitation program was investigated.
Observational, single-centre, and prospective study. Patients referred to cardiac rehabilitation after cardiac surgery, as coronary artery bypass grafting and/or heart valve surgery, with normal left ventricular ejection fraction were enrolled. All patients performed clinical evaluation, traditional and advanced echocardiography, and six-minute walk test before and after cardiac rehabilitation. Individuals enrolled in our study performed aerobic exercise with moderate-intensity continuous training and a program lasting up to 4 weeks with 6 sessions/week.
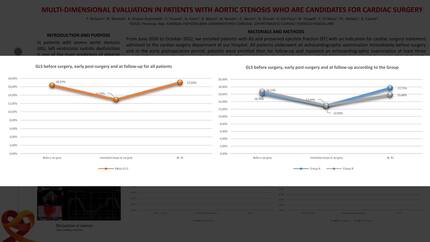
One hundred and one patients with a mean age of 67,86 (± 7,44) years and 68% male were enrolled (table 1). Two- and three-dimensional left ventricular ejection fraction were normal (60,74 ± 5,23% and 60,61 ± 4,79%, respectively) and GLS was reduced (-16,08 ± 2,73%) at baseline assessment. After 4-week intensive cardiac rehabilitation program, GLS and six-minute walk test significantly improved while left ventricular ejection fraction remained preserved (-16,08 ± 2,73% vs -18,24 ± 2,48%, p < 0,001; 68,51 ± 40,26 vs 421,78 ± 120,5 meters, p < 0,001; respectively). Specifically, GLS improved in patients after coronary artery bypass grafting (p < 0,001) and/or aortic valve surgery (p 0,006) but not after mitral valve surgery (p 0,06). Furthermore, baseline GLS was inversely correlated with its delta change (11,73 ± 10,06%) and lower values were associated with greater improvement due to rehabilitation (r2 = -0,601, p < 0,001; figure 1). Finally, an optimal baseline GLS cut-off value of -15,55% predicted an improvement ≥ 11,73%, with a sensitivity of 76% and specificity of 79% (area 0,843; 0,769–0,917; p < 0,001; Youden index 0,541; figure 2), after cardiac rehabilitation.
Cardiac rehabilitation improves subclinical left ventricular dysfunction in patients after cardiac surgery, specifically those undergoing coronary artery bypass grafting and/or aortic valve surgery. Optimal cut-off value of -15,55% for left ventricular GLS predicted improvement of ≥ 11,73%.
Contributors


You may be interested in