Effects of Sacubitril/Valsartan on all-cause hospitalizations in heart failure: participant-level pooled analysis of PARADIGM-HF and PARAGON-HF
European Heart Journal


Abstract
Sacubitril/valsartan is indicated to reduce the risk of cardiovascular (CV) death and heart failure (HF) hospitalizations in patients with chronic HF. However, many of these patients are older and have multiple comorbidities that increase the risk of hospitalizations other than HF, yet the effects of sacubitril/valsartan on hospitalizations of any cause have not been well described.
PARADIGM-HF and PARAGON-HF were phase-3, global multicenter randomized clinical trials that evaluated sacubitril/valsartan versus enalapril (in PARADIGM-HF) or valsartan (in PARAGON-HF) across the spectrum of left ventricular ejection fraction (LVEF; ≤40% in PARADIGM-HF and ≥45% in PARAGON-HF). We pooled individual participant-level data from these 2 trials to examine the effects of sacubitril/valsartan on time-to-first investigator-reported all-cause and cause-specific hospitalization using Cox proportional hazards models, stratified by geographic region and trial. We additionally examined heterogeneity in treatment response by LVEF.
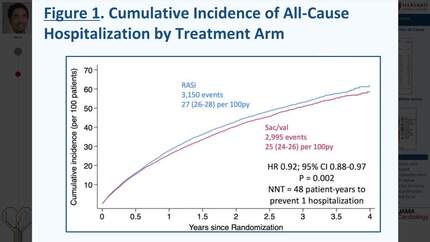
Over 2.8 years median follow-up, among 13,194 participants in the pooled PARADIGM-HF/PARAGON-HF, sacubitril/valsartan significantly reduced the risk of all-cause hospitalizations compared with renin-angiotensin system inhibitor (HR 0.92; 95% CI 0.88-0.97; P=0.002); Figure 1 Panel A. The absolute risk reduction (ARR) was 2.1 per 100 patient-years corresponding to a number-needed-to-treat (NNT) of 48 patient-years of treatment exposure to prevent 1 all-cause hospitalization. Reductions in overall hospitalizations among patients with identifiable causes (N=5,783) seemed to be primarily driven by lower rates of cardiac and pulmonary hospitalizations associated with sacubitril/valsartan. Patients treated with sacubitril/valsartan did not have a higher rate of composite non-cardiac hospitalizations (Figure 1 Panel B). Similarly, sacubitril/valsartan reduced the risk of the composite of all-cause hospitalization or all-cause mortality (HR 0.92; 95% CI 0.87-0.96; P<0.001), with an ARR of 2.5 per 100 patients-years and an NNT of 40 patient-years. For all-cause hospitalization, we observed significant heterogeneity by LVEF as a continuous measure (Pinteraction=0.027); treatment effects were most apparent in those with an LVEF below 60% (HR 0.91 95% CI 0.86-0.96; Figure 2).
In a pooled analysis of >13,000 patients with chronic HF, sacubitril/valsartan reduced hospitalization for any reason with benefits most apparent among those with an LVEF below normal.
Contributors







You may be interested in