Multimodality approach to the no-entry ventricle for VT ablation: first European experience of the RA-to-LV percutaneous access—a case report
European Heart Journal - Case Reports


Abstract
Catheter ablation of ventricular tachycardia (VT) in patients with both mechanical aortic and mitral valves remains challenging, as conventional retrograde or transseptal approaches are not feasible due to the risk of damaging prostheses. Alternative strategies such as thoracotomy, epicardial access, or stereotactic radiotherapy may be unsuitable due to anatomical or technical constraints. The right atrium-to-left ventricle (RA-to-LV) puncture through the inferoseptal process has recently emerged as a potential solution, yet real-world experience remains limited.
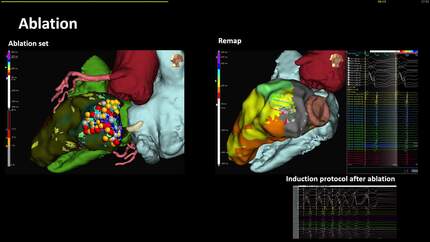
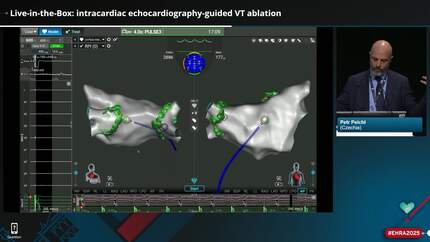
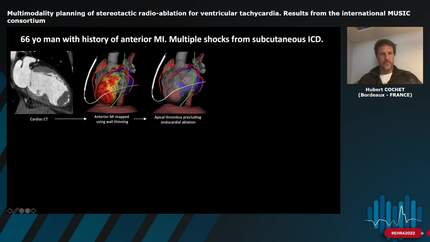
An 81-year-old man with rheumatic heart disease, double mechanical left-sided valve replacement, chronic kidney disease, and recurrent drug-refractory VT was referred for catheter ablation. Multimodal imaging using cardiac magnetic resonance and contrast-enhanced CT processed with ADAS3D software enabled identification of the arrhythmogenic substrate in the basal lateral LV and preprocedural planning of a safe puncture trajectory. Under general anaesthesia and uninterrupted anticoagulation, a percutaneous RA-to-LV puncture was performed with real-time guidance from electroanatomical mapping, CT-fluoroscopy integration, and intracardiac echocardiography. High-density mapping revealed a basal lateral scar with areas of conduction deceleration. Targeted ablation eliminated abnormal potentials and rendered VT non-inducible. A small restrictive iatrogenic Gerbode defect was observed without haemodynamic impact at 4-month follow-up echocardiogram. The patient recovered uneventfully and remained free of VT and ICD therapies at 5-month follow-up.
This case suggests that RA-to-LV access is feasible and safe in a highly selected patient when thorough multimodal planning is undertaken. This report represents the first European experience and supports the potential role of this technique in patients with no-entry ventricle.
Contributors


Julian Rodriguez García
Author

Ignasi Anguera
Author
Paolo Domenico Dallaglio
Author
Stefan Simovic
Author
Sebastian Feickert
Author
Vea Maslova
Author
Lucy Zheng
Author
Deepti Ranganathan
Author
You may be interested in