VA-ECMO in practice: does aetiology matter?
European Heart Journal - Acute CardioVascular Care


Abstract
Peripheral veno-arterial extracorporeal membrane oxygenation (VA-ECMO) is used to provide cardiopulmonary support in patients with refractory cardiogenic shock (CS) or cardiac arrest (CA). Cardiogenic shock aetiologies may be highly heterogeneous. Understanding whether the underlying aetiology influences clinical trajectory and outcomes is key to optimising patient selection and tailoring VA-ECMO strategies.
To analyse the clinical and demographic characteristics of peripheral VA-ECMO patients admitted to our Cardiac Intensive Care Unit (CICU), stratified by aetiology, and to assess differences in outcomes.
We conducted a retrospective observational study of all patients who received VA-ECMO support in our CICU between January 2021 and August 2025. Demographic data, cardiovascular risk factors (CVRF), laboratory biomarkers, and clinical outcomes were collected. Patients were stratified by aetiology, comparing acute coronary syndrome (ACS) vs. non-ACS CS.
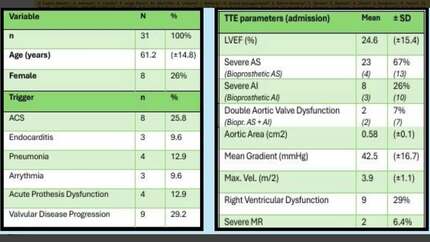
A total of 65 patients were included: 40 with an ACS aetiology (61.5%) and 25 with a non-ACS aetiology (38.5%). Ischaemic patients were more frequently male (87.5% vs. 52%, p=0.002) and older (58.9 vs. 47.8 years, p=0.007). Fewer patients in the ACS group were suitable for full escalation of care (82.5% vs. 100%, p=0.027). ACS patients more often presented with CA requiring extracorporeal cardiopulmonary resuscitation (ECPR) (70% vs. 36%, p=0.007) and had poorer respiratory parameters, including lower PaO2/FiO2 ratio at 24h (210 ±108 vs. 285 ±134, p=0.026). Rates of bleeding, thrombosis and stroke were similar between groups. Univariate analysis showed higher mortality in the ACS group (62.5% vs. 36%, p=0.037). In a multivariate analysis adjusted for age, sex, baseline renal function, ECPR at admission and aetiology, only ECPR at admission was independently associated with mortality.
Patients requiring peripheral VA-ECMO due to ACS CS represent a distinct subgroup, featuring classic high-risk factors such as older age, more frequent CA or worse respiratory course. However, when controlling confounding factors, in our cohort, clinical presentation showed a greater prognosis value than aetiology among peripheral VA-ECMO patients. Clinical characteristics and outcomes Multivariate regression analysis
Contributors

M Brusosa
Author
C Roca-Guerrero
Author
J Llevadot-Sesmilo
Author
G Perez-Domenech
Author
A Martinez-Guisado
Author
E Moreno-Monterde
Author
J Moreno-Coca
Author
E Bechtold-Javier
Author
O Ventosa-Blazquez
Author
I Martinez-Saludes
Author
T Lopez-Sobrino
Author
O De Diego
Author
J T Perez-Ortiz
Author
R Andrea-Riba
Author
You may be interested in