Cardiac sarcoidosis imaging features and latest advances in the management of arrhythmias: a case report
European Heart Journal - Case Reports


Abstract
Cardiac sarcoidosis (CS) is a potentially life-threatening granulomatous inflammatory cardiomyopathy associated with conduction abnormalities, ventricular arrhythmias, and heart failure. Multimodality imaging plays a key role in diagnosis, risk stratification, and guiding therapy.
A 53-year-old male presented with an out-of-hospital ventricular fibrillation arrest in May 2022. Transthoracic echocardiography demonstrated moderate left ventricular (LV) systolic impairment with hypokinesis of the basal inferoseptum, anteroseptal, and basal to mid-inferior walls. Invasive coronary angiography excluded flow-limiting coronary artery disease, and a cardiac resynchronization therapy defibrillator was implanted.
Cardiac magnetic resonance imaging (CMR) was performed in February 2024, but image quality was suboptimal due to device artefact. It showed generalized hypokinesia with thinning and akinesia of the basal to mid-septum; late gadolinium enhancement was present but difficult to characterize. Over the following 18 months, serial CMR and 18F-fluorodeoxyglucose positron emission tomography (PET) demonstrated progressive LV dilatation with worsening LV systolic function, extensive non-ischaemic fibrosis, and intermittent low-grade inflammation.
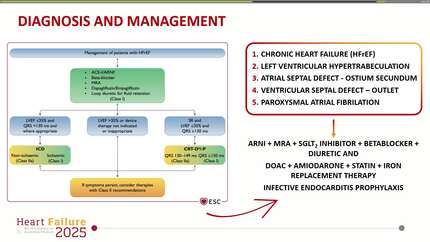
In June 2024, a definite diagnosis of cardiac sarcoidosis was established after discussion at the Sarcoidosis Multidisciplinary Team meeting. Immunosuppression (intravenous methylprednisolone followed by oral prednisolone and methotrexate) achieved partial disease control; however, recurrent ventricular tachycardia persisted despite antiarrhythmic therapy. A PET scan in May 2025 showed stable scar burden with subtle new fluorodeoxyglucose (FDG) uptake in the mid-inferolateral and inferoseptal walls. Given ongoing ventricular tachycardia (VT) and biventricular dysfunction, he was referred for VT ablation and heart transplant assessment.
This case highlights the role of CMR and PET in monitoring CS, differentiating inflammatory from scar-mediated arrhythmias and guiding advanced interventions.
Contributors

Rakesh Sharma
Author
Ana Pericao
Author
Mansimran Singh Dulay
Author
Jonathan M Behar
Author
Andreas Metzner
Author
Christoph Hammerstingl
Author
Deepti Ranganathan
Author