The ‘bystander’ stenosis dilemma: a case against revascularization in a territory of extensive myocardial scar—a case report
European Heart Journal - Case Reports


Abstract
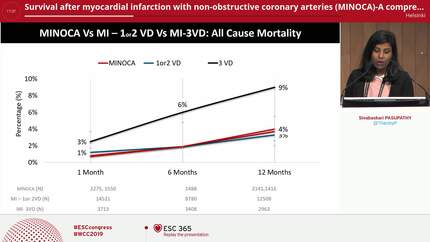
Myocardial infarction with non-obstructive coronary arteries (MINOCA) is a working diagnosis that requires careful exclusion of alternative ischaemic mechanisms. This case highlights a MINOCA mimic: a silently evolved, spontaneously reperfused transmural infarction, where cardiac magnetic resonance (CMR) was decisive for clarifying the mechanism and guiding management.
A 38-year-old man with heavy smoking as his sole cardiovascular risk factor underwent a routine evaluation. ECG demonstrated features of a large anterior infarction, while cardiac biomarkers were negative. Echocardiography showed severe left ventricular dysfunction and a large apical thrombus. Angiography revealed a partially recanalized mid-left anterior descending (LAD) and a severe diagonal stenosis without an obvious culprit lesion. CMR demonstrated a large transmural, non-viable LAD territory infarction with microvascular obstruction. A genetic panel revealed polymorphisms potentially contributing to a prothrombotic condition. Given the absence of viability, revascularization was deferred. At 6-month follow-up, the patient remained asymptomatic, with persistent apical thrombus despite anticoagulation.
Silent, spontaneously reperfused infarction may mimic MINOCA when angiography reveals only mild or intermediate lesions. CMR is essential for identifying non-viable myocardium, avoiding misclassification, and guiding management. Young patients with extensive infarction may benefit from targeted thrombophilia evaluation.
Contributors

You may be interested in