Outcomes of transradial versus transfemoral secondary access in transcatheter aortic valve implantation: a systematic review and meta-analysis
European Heart Journal Supplements


Abstract
Transcatheter aortic valve implantation (TAVI) requires both a primary access route for valve delivery and a secondary access for angiographic visualization. While transfemoral access (TFAC) is conventionally used, transradial access (TRAC) has recently emerged as a promising alternative.
This systematic review and meta-analysis aimed to evaluate the comparative safety and efficacy of TRAC versus TFAC for secondary access in TAVI procedures.
A comprehensive literature search was performed using MEDLINE, Scopus, and the Cochrane Central Register of Controlled Trials databases from their inception through October 1, 2025. Studies comparing TRAC and TFAC for the secondary access for TAVI were included. The primary endpoint was the 30-day all-cause mortality. Secondary endpoints included 30-day stroke, acute kidney injury (AKI), total, life-threatening, and major bleeding events, as well as total, major, and minor vascular complications and the in-hospital length of stay.
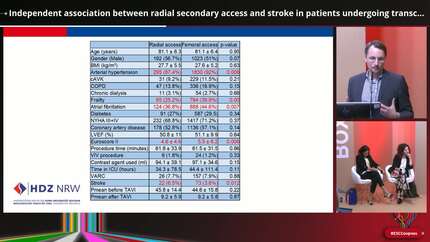
A total of eight studies including15,462 patients (3,319 in the TRAC group and 12,143 in the TFAC group) were included in this meta-analysis. The mean age was comparable between the two groups (81.19±6.67 in TRAC vs 81.53±6.36 years in TFAC). The proportion of females was 44% and 50.1%, respectively. The mean Society of Thoracic Surgeons (STS) score was 4.04±2.9 in the TRAC group and 4.4±2.83 in the TFAC group, while the prevalence of peripheral artery disease was 13.6% and 17.7%, respectively. All-cause mortality was significantly lower in the TRAC group compared with the TFAC group (RR 0.45, 95% CI 0.36–0.57). Both total (RR 0.44, 95% CI 0.30–0.66) and major (RR 0.51, 95% CI 0.30–0.87) bleeding events were significantly lower in the TRAC group, whereas life-threatening bleeding did not differ between the two groups (RR 0.66, 95% CI 0.32–1.34). Furthermore, total (RR 0.47, 95% CI 0.25–0.89) and major (RR 0.45, 95% CI 0.27–0.73) vascular complications were lower in the TRAC group, while minor vascular complications showed no significant difference between the two approaches. Finally, no significant difference was observed in 30-day stroke rates (RR 0.68, 95% CI 0.45–1.02), while the incidence of 30-day AKI was significantly reduced in the TRAC group (RR 0.48, 95% CI 0.38–0.60).
The findings of our meta-analysis indicate that the TRAC secondary access route in TAVI is associated with bettersafety outcomes compared with the TFAC, as it was associated with lower rates of all-cause mortality, vascular complications and bleeding. According to our findings, TRAC should be preferred as secondary access. Nevertheless, randomized studies are required to validate ourfindings and establish definitive clinical recommendations.
Contributors


A Apostolos
Author
Royal Brompton Hospital London , United Kingdom of Great Britain & Northern Ireland


K Konstantinou
Author
Harefield Hospital, Royal Brompton and Harefield NHS Foundation Trust London , United Kingdom of Great Britain & Northern Ireland



V Panoulas
Author
K Tsioufis
Author

You may be interested in