Regional differences in patients recruited for ICD/CRT-D therapy across 15 countries from Africa, Middle East, Eastern Europe and CIS countries
European Heart Journal


Abstract
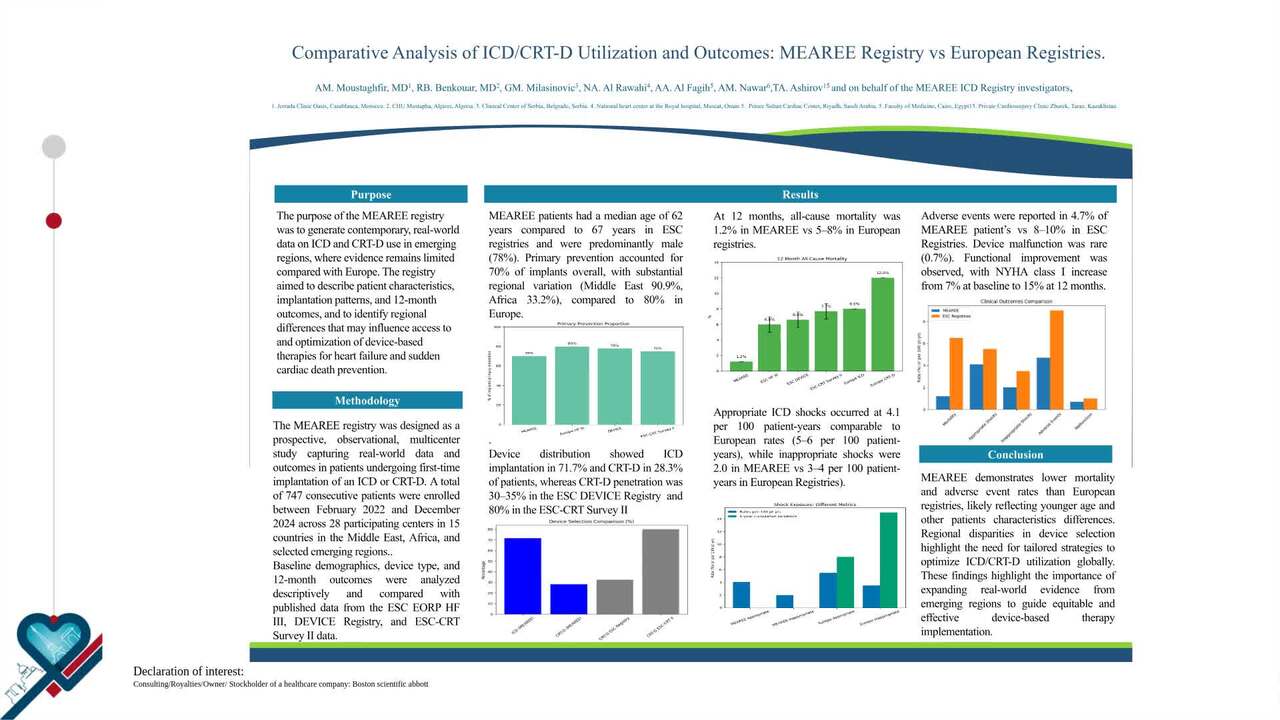
Implantable Cardioverter Defibrillators (ICDs) and Cardiac Resynchronization Therapy Defibrillators (CRT-Ds) are established therapies in patients with heart failure and at risk of sudden cardiac death (SCD). Extensive registries and comprehensive data analysis have been conducted in the United States and Western Europe, but data are scarce in other geographies.
The MEAREE ICD registry aimed to collect data about baseline characteristics of patients receiving ICDs and CRT-Ds in Middle East, Africa, East Europe (EE), and Commonwealth of Independent States countries (CIS).
Twenty-seven Cardiology Departments in 15 countries prospectively collected clinical and device data in ICD/CRT-D patients. Here we reported data about patients baseline characteristics.
A total of 751 patients (162 females, mean age 63 ± 13 years) were included in the study between February 2022 and October 2023 and followed for 12 months. Implant indication was SCD primary prevention 73.6% and secondary prevention 26.4%. Primary Prevention was highest in the Middle East (90.9%), CIS and EE (86.8%), with Africa at 33.2%. The implantation procedures were successful in 100% of cases, with ICDs accounting for 71.7% and CRT-Ds for 28.3%. The percentage of patients with ICDs was highest in CIS (80.8%), followed by Africa (76.9%) and the Middle East (54%). Insurance coverage varied significantly, with government insurance being the most common in all regions (62.9% in Africa, 87.5% in the Middle East, and 97.8% in CIS and EE). NYHA Class II was the most prevalent in Africa (63.7%) and the Middle East (64.7%), while NYHA Class III was most common in CIS and EE (67.6%). Prior myocardial infarction was highest in CIS (51.6%) and prior percutaneous coronary intervention was highest in the Middle East (35.3%). Non-ischemic hypertensive heart disease was significantly more common in the Middle East (31.7%) compared to Africa (4.3%) and CIS & EE (6.6%). The study also highlighted differences in smoking status, with the highest percentage of active smokers in the Middle East (26.8%) and the highest percentage of ex-smokers in Africa (40%). The prevalence of hypertension was highest in CIS & EE (76.7%), while diabetes mellitus was most common in the Middle East (62%). The mean LVESV was 103 ± 90 ml in Africa, 104 ± 63 ml in the Middle East, and 117 ± 69 ml in CIS and EE. The mean LVEF was 33 ± 14% in Africa, 28 ± 10% in the Middle East, and 32 ± 9% in CIS and EE. The characteristics varied significantly across regions, revealing notable differences in patient demographics and comorbidities.
This study shows differences in 15 countries from Africa, Middle East, Eastern Europe and CIS in ICD/CRT-D utilization and patient characteristics. Improving knowledge about regional specificities might improve patient care quality across various regions.
Contributors


R B Benkouar
Author
G M Milasinovic
Author
N A Al-Rawahi
Author
A A Al Faghih
Author
A N Nawar
Author
V R Barsukevitch
Author
A H Haggui
Author
N M Maharaj
Author
O K Kamel
Author
H M Rasmy Mohamed
Author
M K Khoury
Author
A G Grammatico
Author
T A Ashirov
Author
You may be interested in