Global left ventricular myocardial work efficiency in left bundle branch pacing versus right ventricular pacing: results of an observational study. An extended 2-year follow up
European Heart Journal


Abstract
Right ventricular pacing (RVP) is known to induce electrical and mechanical dyssynchrony, increasing the risk of heart failure and pacing-induced cardiomyopathy. Left bundle branch area pacing (LBBAP) has emerged as a physiological alternative. Recent studies have demonstrated that LBBAP results in higher global myocardial work efficiency (GWE) and improved Left Ventricle contractility compared to RVP. While His-bundle pacing (HBP) has also been explored for conduction system pacing, LBBAP is preferred due to more stable pacing thresholds and reliable lead positioning.
The aim of this study was to compare the effects of LBBAP and RVP on myocardial work efficiency and left ventricular ejection fraction (LVEF%) in patients requiring RVP and LBBAP.
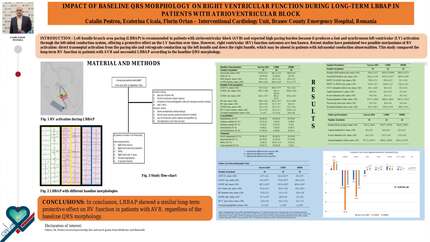
This was a prospective observational study including patients with atrioventricular block (AVB) and preserved EF who underwent either LBBAP or RVP. Patients were divided into two groups: LBBAP (N = 34) and RVP (N = 29). Three patients in the LBBAP group were classified as left ventricular septal pacing (LVSP), one patient required crossover to RVP due to failure to achieve conduction system capture. Echocardiographic parameters, including LVEF% and GWE%, were evaluated before and after implantation. The mean follow-up duration was 2.04 ± 0.94 years.
LVEF before implantation was similar between groups (57.19 ± 4.46% in LBBAP vs. 58.50 ± 4.12% in RVP, p = 0.403). After implantation, LBBAP resulted in significantly higher LVEF compared to RVP (58.39 ± 4.73% vs. 52.35 ± 6.64%, p = 0.002). GWE% was significantly higher in the LBBAP group compared to RVP (85.23 ± 6.82% vs. 80.00 ± 9.41%, p = 0.019). No significant differences were observed in gender distribution (p = 0.302) or comorbidities. Hypertension (p = 0.001) and dyslipidemia (p = 0.116) were more prevalent in the RVP group. No complications during the acute perioperative phase and the running period of the follow-up. Pre-implantation GWE values would not be accurate as the patients presented with atrioventricular block.
LBBAP demonstrated superior preservation of left ventricular systolic function compared to RVP, as evidenced by significantly higher LVEF and GWE after implantation. These results correspond to an extended follow-up of a previous study and demonstrate further divergence of the values in LVEF and GWE, which implies that LBBAP is a pacing strategy that decreases the risk of pacing induced cardiomyopathy.
Contributors




You may be interested in