Size-dependent efficacy of low-voltage area ablation in persistent atrial fibrillation: a subanalysis of the SUPPRESS-AF trial
European Heart Journal


Abstract
A larger low-voltage area (LVA) in the left atrium is associated with an increased risk of arrhythmia recurrence after atrial fibrillation (AF) ablation. Therefore, the efficacy of LVA ablation may differ depending on LVA size.
This study aimed to investigate the impact of LVA size on the efficacy of LVA ablation in patients with persistent AF patients and left atrial LVAs.
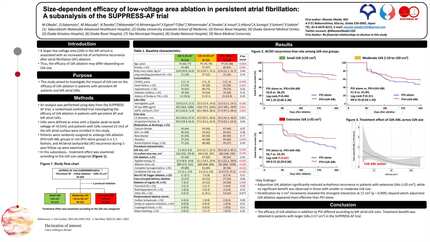
An analysis was performed using data from the SUPPRESS-AF trial, a randomized controlled trial investigating the efficacy of LVA ablation in patients with persistent AF and left atrial LVAs. LVAs were defined as areas with a bipolar peak-to-peak voltage of <0.5mV, and patients with LVAs covered ≥5 cm² of the left atrial surface were enrolled in this study. Patients were randomly assigned to undergo LVA ablation (PVI+LVA-ABL group) or not (PVI-alone group) in a 1:1 fashion. AF/atrial tachycardia (AT) recurrence rate and treatment effect during 1-year follow-up were examined according to the LVA size categories: small LVA (5-10 cm², n=116), moderate LVA (10-20cm², n=121), and extensive LVA (>20 cm², n=107).
The median LVA was 13.4 cm² (interquartile range, 8.7-23.3). The overall incidence of AF/AT recurrence did not significantly differ between the PVI+LVA-ABL and PVI-alone groups (36.3% vs. 41.5%, log-rank p=0.31). Similar results were observed in patients with small LVAs (34.0% vs. 29.3%, log-rank p=0.53) and moderate LVAs (44.4% vs. 41.8%, log-rank p=0.68). However, in patients with extensive LVAs, the recurrence rate was significantly lower in the PVI+LVA-ABL group than PVI-alone group (31.3% vs. 50.9%, log-rank p=0.038). When stratified in 1cm² increments, the treatment effect differed across LVA sizes, with the most significant interaction observed at an LVA of 17 cm² (interaction p=0.023).
The efficacy of LVA ablation in addition to PVI differed according to left atrial LVA sizes. Treatment benefit was obtained in patients with extensive LVAs in the SUPPRESS-AF trial. Kapalan-Meier curves Hazard ratio across LVA spectrum




You may be interested in