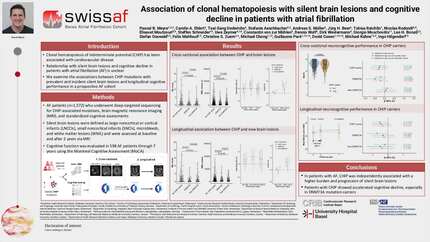
Association of clonal hematopoiesis with silent brain lesions and cognitive function in patients with atrial fibrillation
European Heart Journal


Abstract
Clonal hematopoiesis of indeterminate potential (CHIP) has been implicated in various cardiovascular diseases. However, the association of CHIP with clinically silent brain lesions and cognitive function in patients with atrial fibrillation (AF) is unclear.
This study investigated whether CHIP mutations are associated with prevalent and incident silent brain lesions and longitudinal neurocognitive performance in a prospective AF cohort.
We analyzed 1,572 participants from the Swiss-AF study with targeted sequencing for CHIP-related mutations, brain magnetic resonance imaging (MRI), and standardized neurocognitive testing. Deep sequencing was performed to screen the entire genes for CHIP mutations at baseline. Large noncortical or cortical infarcts (LNCCIs), small noncortical infarcts (SNCIs), microbleeds, and white matter lesions (WML) were assessed at baseline and after 2 years. Cognitive function was evaluated over an 8-year follow-up using the Montreal Cognitive Assessment (MoCA) and the Swiss-AF Cognitive Construct (CoCo) score.
CHIP mutations were present in 342 (22%) patients, with DNMT3A (49.4%) and TET2 (28.3%) being the most frequent. Compared to non-CHIP carriers, those with CHIP mutations had a significantly higher prevalence of SNCIs (Non-CHIP: 19.9%, DNMT3A: 22.2%, TET2: 27%, other genes: 32.3%; Pχ²=0.017), microbleeds (Non-CHIP: 19.9%, DNMT3A: 23.2%, TET2: 33.8%, other genes: 32.7%; Pχ²=0.002), and WML (Non-CHIP: 50.4%, DNMT3A: 61.3%, TET2: 73%, other genes: 68.7%; Pχ²<0.001). Multivariable regression revealed that CHIP is associated with increased odds of microbleeds (odds ratio (OR) = 1.45, 95% CI = [1.09-1.93], P=0.010) and WML (OR = 1.56, 95% CI = [1.20-2.04], P=0.001). In particular, mutations other than DNMT3A/TET2 were associated with SNCI (OR = 1.63, 95% CI = [1.02-2.54], P=0.03), microbleeds (OR = 1.70, 95% CI = [1.07-2.65], P=0.021), and WML (OR = 1.70, 95% CI = [1.07-2.74], P=0.03). Over the 2-year follow-up, patients with non-DNMT3A/TET2 CHIP mutations were at increased risk for new LNCCI (OR = 3.21, 95% CI = [1.03-8.35], P=0.030) and microbleeds (OR = 2.08, 95% CI = [1.07-3.78], P=0.020). CHIP carriers had no significant accelerated decline in cognitive function after adjustment (MoCA: beta = -0.08, 95% CI = [-0.29-0.13], P=0.47; CoCo: beta = -0.01, 95% CI = [-0.04-0.01], P=0.39).
CHIP is associated with a greater burden of silent brain lesions, particularly among patients with non-DNMT3A/TET2 mutations, but does not independently predict cognitive decline in patients with AF.
Contributors



A S M Mueller
Author
A S Stauber
Author

S S Schneider
Author

M K Kuehne
Author
C S Z Zuern
Author
M C Chong
Author

D C Conen
Author
I H Hilgendorf
Author
You may be interested in