Degenerative mitral regurgitation due to flail leaflet: sex-related differences in presentation, management, and outcomes
European Heart Journal


Abstract
Presentation, outcome, and management of females with degenerative mitral regurgitation (DMR) are undefined. We analysed sex-specific baseline clinical and echocardiographic characteristics at referral for DMR due to flail leaflets and subsequent management and outcomes.
In the Mitral Regurgitation International Database (MIDA) international registry, females were compared with males regarding presentation at referral, management, and outcome (survival/heart failure), under medical treatment, post-operatively, and encompassing all follow-up.
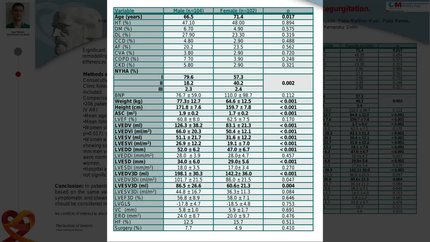
At referral, females (
Females with severe DMR were referred to tertiary centers at a more advanced stage, incurred higher mortality and morbidity under conservative management, and were offered surgery less and later after referral. Ultimately, these sex-related differences yielded persistent excess mortality despite surgery in females with DMR, while males enjoyed restoration of life expectancy, warranting imperative re-evaluation of sex-specific DMR management.
Contributors

Christophe Tribouilloy
Author
Francesca Bursi
Author
Francesco Grigioni
Author
Jean-Louis Vanoverschelde
Author
Noémie Resseguier
Author

Agnes Pasquet
Author
Julie Pradier
Author


Hector Michelena
Author
Giovanni Benfari
Author
Dan Rusinaru
Author
Stéphane Zaffran
Author
David Vancraeynest
Author
Fréderic Collart
Author


Maurice Enriquez-Sarano
Author
You may be interested in