Anatomical-based percutaneous left stellate ganglion block in patients with refractory electrical storm: efficacy and safety
European Heart Journal


Abstract
The autonomic system plays a pivotal role in ventricular arrhythmogenesis. Percutaneous stellate ganglion block (PSGB) is a technique known since many years for analgesic purposes, which has recently proven its antiarrhythmic effect suitable for an emergency setting. However, evidences are limited and heterogeneous.
To assess the efficacy and safety of PSGB performed with an anterior paratracheal approach using anatomical landmarks in consecutive patients with electrical storm refractory to conventional treatment.
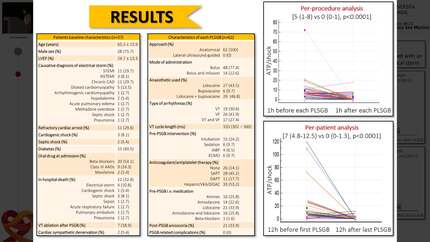
Patients with electrical storm were consecutively enrolled from November 2017 to January 2022. Left PSGB (PLSGB) was performed after failure of at least one intravenous antiarrhythmic drug. Its repetition or a continuous infusion of the local anaesthetic were considered in selected cases. Clinical data, the characteristics of the block and the occurrence of complications were collected. The efficacy was evaluated by comparing the number of arrhythmias treated with ATP or DC-shocks by external or internal defibrillator in the hour before the block with that in the hour after the procedure. Per-patient efficacy was assessed by comparing the number of ATP/shocks in the 24 hours before the procedure with that in the 24 hours after the last procedure.
28 patients were enrolled: 78% male, mean age 65.4±14.2 years; 9 with dilated cardiomyopathy, 8 with chronic ischemic heart disease, 7 with ST-elevation myocardial infarction, 2 with non-ST-elevation myocardial infarction, 1 with arrhythmogenic right ventricular dysplasia and 1 with drug intoxication; the average ejection fraction was 24.2±15%. A total of 44 PLSGBs were performed: 18 for ventricular tachycardia (VT), 11 for ventricular fibrillation (VF) and 15 for both VT and VF episodes; 7 on intubated patients, 3 in extracorporeal circulation, 7 in cardiogenic/septic shock, 22 on patients on single antiplatelet therapy, 7 on dual antiplatelet therapy, 25 on anticoagulant therapy. PLSGBs were performed during intravenous infusion of antiarrhythmics (amiodarone in 24, lidocaine in 27 procedures). The local anaesthetic used was lidocaine 200 mg in 16/44 PLSGB, bupivacaine 50 mg in 4/44 and both in 24/44. The per-procedure analysis showed a significant reduction of the number of ATP/shocks in the hour after PLSGB compared with the hour before [0 (0–0) vs 5 (1–8) p<0.001]. Similarly, in the per-patient analysis, the number of ATP/shocks significantly decreased in the 24 hours after the PLSGB compared with that in the 24 hours before [0 (0–1.5) vs 6.5 (4.5–15.5) p<0.001]. No complications occurred.
This is the largest case series so far in which PLSGB has proven to be highly effective and safe in the treatment of challenging patients with refractory electrical storm. Its safety and the exiguity of the equipment required for the anatomical approach make PLSGB a technique that can be easily performed by cardiologists at the bedside.
Type of funding sources: None.
Contributors

S Compagnoni
Author
F R Gentile
Author
E Baldi
Author
A Sanzo
Author
R Rordorf
Author
S Savastano
Author
You may be interested in