References
Suggested reading:
Rozenbaum Z et al. Discriminating circulatory problems from deconditioning: Echocardiographic and cardiopulmonary exercise test analysis. Chest. 2017;151:431-440.


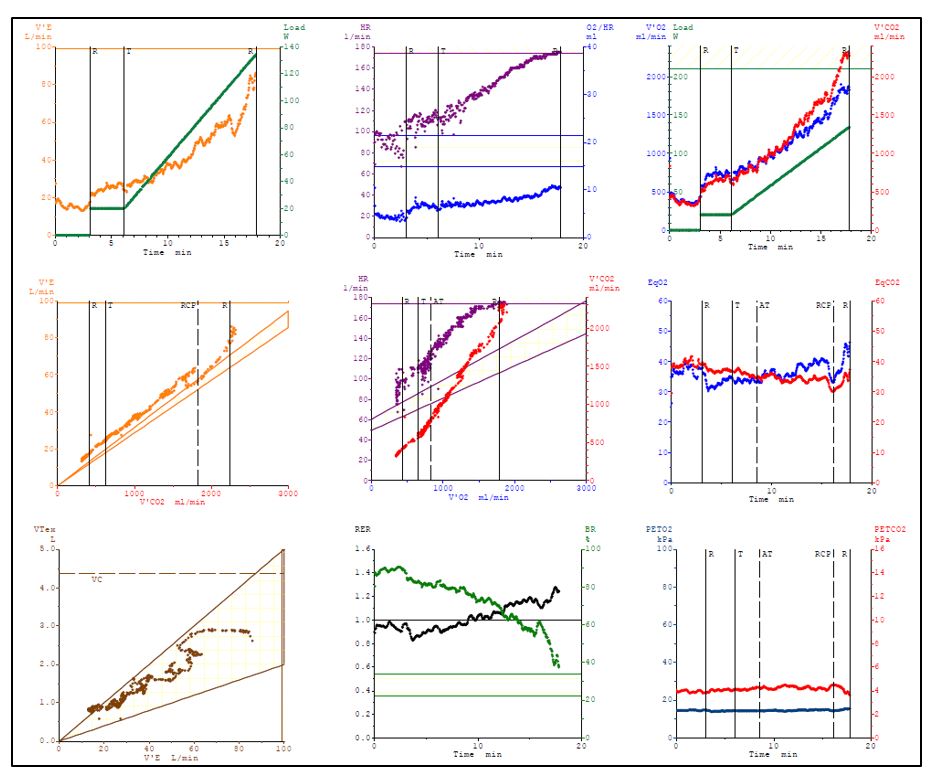
A 36-year-old male cancer patient (BMI 26.8 kg/m2) was assessed with a cardiopulmonary exercise test prior to his cardio-oncology rehabilitation programme:
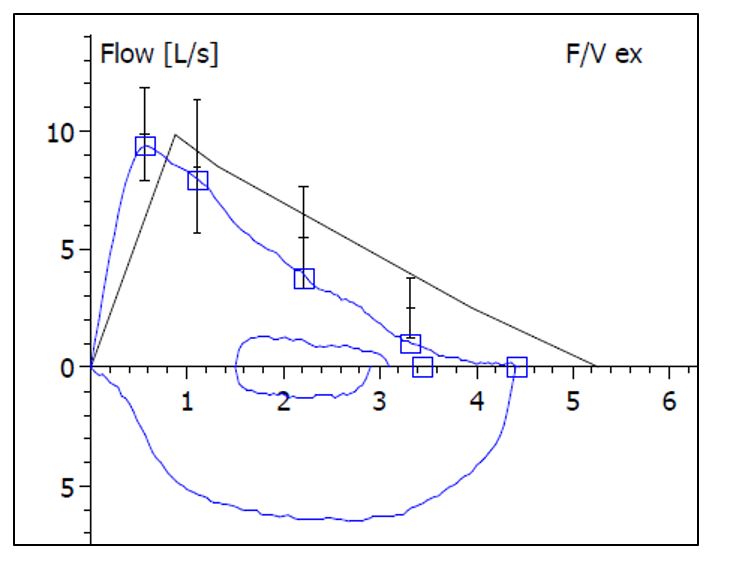
The resting spirometry showed a FVC (forced vital capacity) of 4.4 l (84% predicted), a FEV1 (forced expiratory volume) of 3.4 l (79% predicted), and a FEV1/FVC of 78%. Estimated maximum voluntary ventilation (MVV, FEV1*40) was 137 l/min.
Cardiorespiratory fitness was reduced with a peak VO2 of 20.5 ml/min/kg (58 % predicted) (Panel 3).
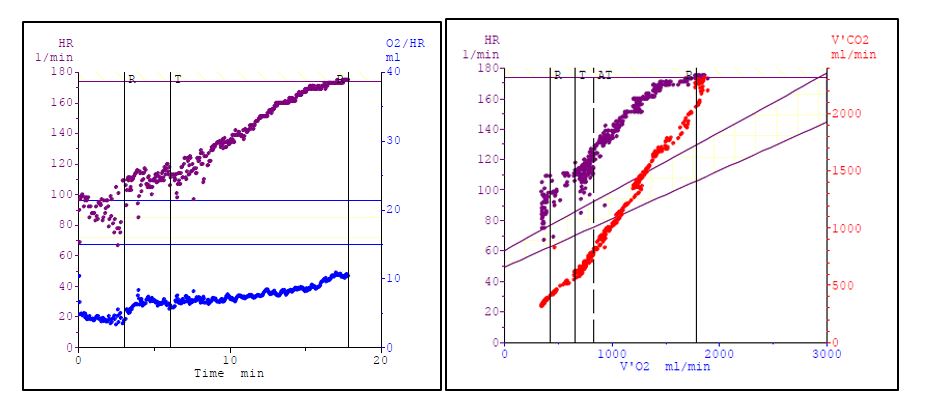
Blood pressure increased from 130/80 mmHg to 165/80 mmHg at peak exercise. Heart rate increased from 109 bpm to 173 bpm (94% of predicted) (Panel 2). Maximum respiratory exchange ratio was 1.23 (Panel 8). The patient was exhausted at the end of the test (Borg 19/20) and complained of exertional dyspnoea.
Maximum ventilation was 81 l (Panel 1). Breathing reserve ((1-VEmax/MVV)*100) was 41% (Panel 8). Respiratory efficiency, determined by the VE/VCO2 slope was 33 (Panel 4). The O2 pulse (VO2/heart rate) increased to 10.6 ml (59% of predicted, Panel 2). The VO2/work rate trajectory was 9.4 ml/min/watt (Panel 3).
Suggested reading:
Rozenbaum Z et al. Discriminating circulatory problems from deconditioning: Echocardiographic and cardiopulmonary exercise test analysis. Chest. 2017;151:431-440.