Case report: combined transcatheter paravalvular leak closure and valve-in-valve transcatheter aortic valve replacement for treatment of severe regurgitation complicating transcatheter aortic valve replacement
European Heart Journal - Case Reports


Abstract
Concurrent transvalvular regurgitation (TVR) and paravalvular leak (PVL) complicating transcatheter aortic valve replacement (TAVR0 is rare, and optimal management is not well described.
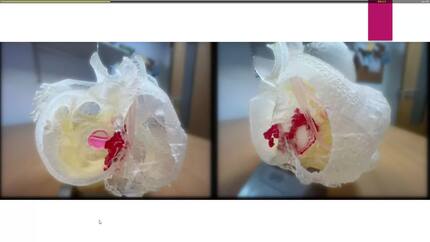
A 74-year-old man with LVEF of 40% and prior TAVR (34-mm Medtronic Evolut) presented 8 years post-implantation with New York Heart Association (NYHA) class IV acute decompensated heart failure. Transthoracic echocardiography (TTE) identified severe bioprosthetic aortic regurgitation; transoesophageal echocardiography (TEE) delineated concomitant severe TVR and PVL. Computed tomographic angiography (CTA) identified a discrete paravalvular tunnel between two calcific annular nodules. Given the prohibitive surgical risk, he underwent single-session transcatheter PVL closure with an Amplatzer ductal occluder followed by valve-in-valve TAVR with an Edwards SAPIEN 3 Ultra RESILIA valve. AR pressure half-time improved from 217 to 436 ms, and invasive aortic diastolic pressure normalized from approximately 40–65 mm Hg. At 30-day follow-up, symptoms had improved to NYHA class II, with trace residual PVL and no TVR on TTE.
To the best of our knowledge, this represents one of the first reported cases of a combined single-session percutaneous approach, consisting of transcatheter PVL closure and valve-in-valve TAVR, to address mixed-mechanism bioprosthetic aortic regurgitation. TEE and CTA are essential for mechanism delineation. A combined transcatheter approach is feasible and effective in high-risk patients.
Contributors

Luca Halalau
Author
Luai Madanat
Author
Ivan Hanson
Author
Can Gollmann-Tepeköylü
Author
Erick Alexanderson Rosas
Author
Ahsan Aftab Khan
Author
Damiano Regazzoli-Lancini
Author
Deepti Ranganathan
Author
You may be interested in