Comparative analysis of 6-lead and single-lead consumer-grade electrocardiograms: diagnostic accuracy, numerical agreement, and inter-rater reliability
European Heart Journal - Digital Health


Abstract
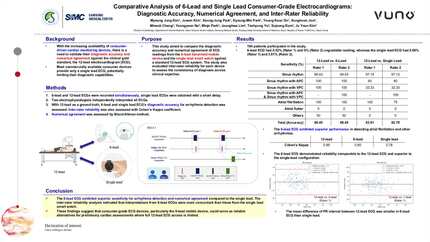
Consumer-grade electrocardiogram (ECG) devices enable accessible rhythm monitoring. Recently developed six-lead handheld ECGs promise improved signal quality and diagnostic performance; however, comparative validation remains limited. Using 12-lead ECGs as reference, we compared diagnostic performance and quantitative agreement of a 6-lead and single-lead consumer ECGs.
In this prospective single-centre study, 194 arrhythmia-clinic patients (498 paired recordings) underwent simultaneous 10-s 12-lead and 30-s 6-lead ECG acquisition, followed by sequential 30-s single-lead recording. Two blinded electrophysiologists interpreted ECGs. Diagnostic performance for predefined rhythm categories (sinus rhythm, atrial/ventricular premature complex, atrial fibrillation/flutter/tachycardia, atrioventricular block, others) was assessed by sensitivity, specificity, and accuracy. Waveform agreement was evaluated using Bland–Altman analysis and intraclass correlation coefficients (ICC) accounting for repeated measures. Sensitivity was higher for the 6-lead ECG for ectopic beats, atrial flutter, and first-degree atrioventricular block, with comparable specificity across categories. Overall diagnostic accuracy was 98.6% (95% confidence interval, 97.4–99.6) for the 6-lead and 96.9% (94.7–98.7) for the single-lead ECG. Agreement with the 12-lead ECG was higher for the 6-lead device for PR interval (ICC 0.89; 0.85–0.92) and QRS amplitude (0.96; 0.94–0.97) than for the single-lead device (0.57; 0.48–0.63 and 0.04; −0.13–0.21, respectively). Bland–Altman analysis demonstrated generally narrower limits of agreement for the 6-lead ECG. Findings were consistent in patient-level sensitivity analyses.
The 6-lead handheld ECG demonstrated a higher point estimate for diagnostic accuracy and closer agreement with the 12-lead ECG than the single-lead smartwatch ECG, supporting its use for arrhythmia assessment and interval measurement.
Contributors

Juwon Kim
Author
Seung-Jung Park
Author
Kyoung-Min Park
Author
Young Keun On
Author

Mineok Chang
Author
Myoung Jung Kim
Author
Yeongyeon Na
Author
Minje Park
Author
Jeonghwa Lim
Author
Taehyung Yu
Author
Hyun Jin Ahn
Author
Ju Youn Kim
Author
You may be interested in