Post-procedural computed tomography comparison of predicted and actual neo-left ventricular outflow tract after one-session double valve-in-valve implantation: a case report
European Heart Journal - Case Reports


Abstract
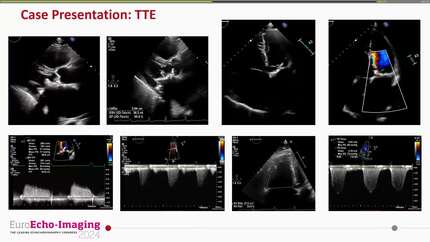
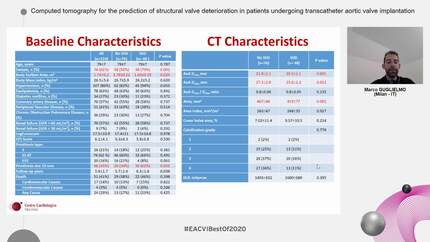
Left ventricular outflow tract (LVOT) obstruction is a serious complication of transcatheter mitral valve replacement and mitral valve-in-valve (ViV) procedures. Computed tomography (CT)-based virtual valve implantation predicts the neo-LVOT area, but it assumes idealized seating and may not fully reflect procedural interaction during double-valve intervention.
A 74-year-old woman with degenerated surgical mitral and aortic bioprostheses presented with NYHA class IV heart failure. Full-cycle ECG-gated 4D-CT identified the minimum predicted neo-LVOT at 43% of the R–R interval (300.9 mm2). A one-session transapical double ViV procedure was performed. The aortic ViV was performed first because CT simulation showed that the aortic balloon would expand between the two strut posts of the surgical mitral prosthesis; implanting the mitral valve first could have exposed the newly deployed mitral prosthesis to compression during subsequent aortic balloon expansion. Post-procedural 4D-CT, evaluated using the same workflow and compared at 43%, showed a neo-LVOT area of 280.6 mm2, a 20.3 mm2 reduction, with approximately 1.2 mm asymmetric ventricular protrusion of the mitral prosthesis. Echocardiography showed normal valve-in-valve function and no haemodynamic LVOT obstruction.
This case demonstrates that CT-based planning correctly identified procedural feasibility, while post-procedural CT revealed measurable geometric variability. The finding remained well above high-risk thresholds and should be interpreted as a hypothesis-generating geometric observation rather than clinically significant obstruction.
Contributors

Weili Liu
Author
Ju Zhang
Author
Kai Zhang
Author
Yanchao Li
Author
Dacheng Li
Author
Christoph Sinning
Author
Deepti Ranganathan
Author
You may be interested in