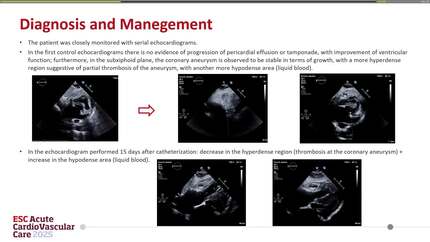
A case with suspected ruptured mycotic coronary aneurysm presenting as purulent bloody pericarditis
European Heart Journal - Case Reports


Abstract
Coronary artery aneurysms are rare, and mycotic coronary aneurysms arising secondary to bacterial infection are even rarer.
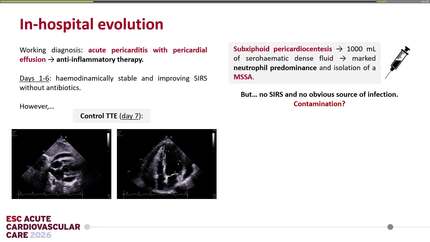
A 77-year-old woman with end-stage renal disease presented with a 1-week history of persistent fever following arteriovenous fistula creation. Transthoracic echocardiography revealed a mild pericardial effusion. On the day after admission, a blood culture yielded methicillin-sensitive
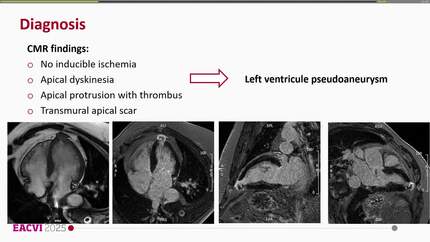
Autopsy studies have revealed that most mycotic coronary aneurysms represent ‘pseudoaneurysms’, characterized by thinning of the arterial wall with outward bulging due to disruption of the elastic tissue layers. Thus, rapid dilation of the aneurysm and eventual rupture into the pericardial cavity may be key characteristics of this pathological condition. Clinicians should maintain a high index of suspicion for mycotic coronary aneurysms in patients with persistent bacteraemia and pursue prompt multimodal imaging for early detection, particularly when the standard evaluations for infective endocarditis are unknown. Furthermore, in the presence of haemorrhagic pericardial effusion, timely surgical intervention is imperative, because it indicates aneurysmal rupture.
Contributors

Koji Kashiki
Author

Akitoshi Yamada
Author
Satoru Kawasaki
Author
Hogara Nishisaki
Author
Timothy C Tan
Author
Sarv Priya
Author
Naoki Arima
Author
Dimitrios Karelas
Author
You may be interested in