Trauma-triggered coronary embolism causing extensive anterolateral ST-segment elevation myocardial infarction in a young man with a mechanical aortic valve: a case report
European Heart Journal - Case Reports


Abstract
Coronary embolism is a rare but clinically important non-atherosclerotic cause of acute myocardial infarction. Its diagnosis becomes especially challenging in young patients with mechanical valves, especially when the presentation follows blunt chest trauma.
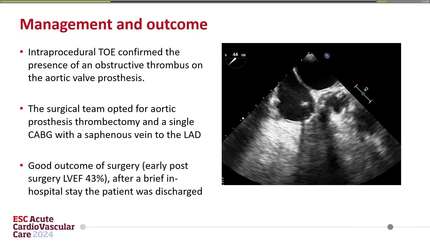
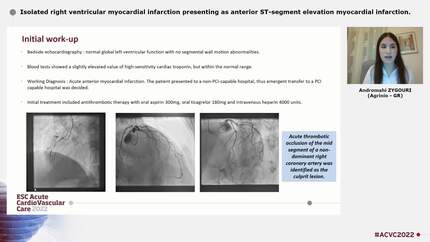
A 24-year-old man with a mechanical aortic valve presented with progressive chest pain and dyspnoea 2 days after blunt chest trauma. Electrocardiography (ECG) demonstrated extensive anterior–lateral ST-segment elevation myocardial infarction (STEMI). Transoesophageal echocardiography revealed normal prosthetic valve function, an apical aneurysm, and a non-mobile left ventricular (LV) mural thrombus. Coronary angiography showed a large thrombotic occlusion in the proximal left anterior descending (LAD) artery with otherwise normal coronary anatomy. Findings were most consistent with coronary embolism originating from a trauma-induced LV mural thrombus. Given the high thrombus burden, the patient received dual antiplatelet therapy, continued warfarin, and tirofiban infusion. Follow-up imaging confirmed complete resolution of the thrombus and improvement in ventricular function.
This case illustrates the rare mechanism of trauma-induced LV mural thrombus embolization causing STEMI in a young prosthetic-valve patient. Integration of multimodality imaging coupled with meticulous clinical reasoning is required for systematic exclusion of spontaneous coronary artery dissection (SCAD), infective endocarditis, prosthetic-valve thrombosis, hypercoagulable states, and
Contributors

Davar Aledavood
Author
Zahra Alizadeh
Author
Krishnaraj Rathod
Author
Samah Ismael Abohamr
Author
Jabir Abdullakutty
Author
Deepty Ranganathan
Author
You may be interested in