Outcomes of simplified left atrial appendage occlusion using the WATCHMAN FLX device: the ROSE-FLX study
EP Europace Journal


Abstract
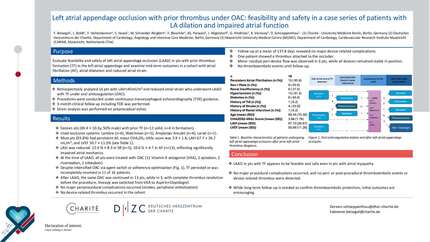
Conventional left atrial appendage occlusion (LAAO) procedures typically require transoesophageal echocardiography and general anaesthesia, which may limit feasibility in resource-limited settings. Simplified LAAO (sLAAO) guided exclusively by fluoroscopy offers a practical and efficient alternative. This study evaluated procedural safety, efficacy, and short-term outcomes of sLAAO using the WATCHMAN FLX device under exclusive fluoroscopic guidance in a real-world, multicentre setting.
The ROSE-FLX study was a prospective, multicentre, single-arm registry including 400 patients with non-valvular atrial fibrillation at high thromboembolic and bleeding risk. All underwent sLAAO under local anaesthesia and exclusive fluoroscopic guidance. Procedural data, peri-procedural complications, and follow-up outcomes were analysed. Predictors of adverse events were determined using Cox regression. Procedural success was 100%, with low major complication rates: pericardial effusion (0.5%), access-site complications (1.3%), and major bleeding (0.8%). Over median follow-up of 194.5 days [interquartile range (IQR) 129.0–265.0], all-cause mortality occurred in three patients (0.8%), transient ischaemic attacks in 13 patients (3.3%), and device-related thrombosis in one patient (0.3%). In multivariable Cox regression, chronic obstructive pulmonary disease (HR 2.86, 95% CI 1.98–4.11,
Exclusive fluoroscopy-guided sLAAO with the WATCHMAN FLX device is feasible, safe, and resource efficient, achieving high procedural success and low complication rates, suggesting that this approach may be considered in selected centres lacking advanced echocardiographic or anaesthetic support, pending confirmation from comparative studies.
Contributors

Wei Zhou
Author
Qian Tang
Author
Anning Zeng
Author
Jiulin Chen
Author
Fang Wang
Author
Jing Wang
Author
Jingjing Chen
Author
LinYan Shi
Author
Ji Li
Author
Yirong Zhang
Author
Dawei Tian
Author
Dandan Chen
Author
Fuliang Luo
Author
Zheyi Wu
Author
Na Deng
Author
Fei Yan
Author
Qianjiang Pan
Author
Zhongrong Liao
Author
Yongxian Tian
Author
Yifan Mao
Author
Huimin Lu
Author
Xing Zhou
Author
Ya Yang
Author
ZhenFa Zhang
Author
Runze Huang
Author
Wei Li
Author
You may be interested in