Heart failure and tricuspid regurgitation: the role of SGLT2 inhibitors in improving outcomes Insights from SHEBAHEART big data registry
European Heart Journal - Cardiovascular Pharmacotherapy


Abstract
Sodium-glucose cotransporter-2 inhibitors (SGLT2i) have transformed heart failure (HF) management, yet their effect in patients with concomitant tricuspid regurgitation (TR) remains unclear. We evaluated the association of SGLT2i use with clinical outcomes in HF patients with and without TR.
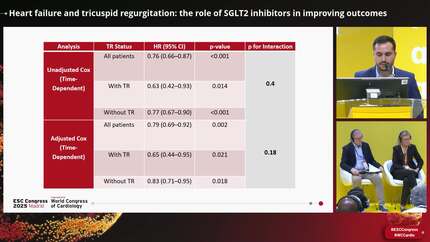
We analysed a cohort of patients with HF (2014–2024) who underwent echocardiography within 90 days of diagnosis. Patients were stratified by significant TR and SGLT2i use. The primary outcome was a composite of all-cause mortality and HF hospitalization. TR progression was a secondary outcome. Inverse probability treatment weighting and time-dependent Cox models were used to adjust for baseline and treatment differences. Among 28 940 HF patients [median age 75 (IQR 66–83), 43% women], 4043 (14%) had significant TR, and 2320 (8%) received SGLT2i. Over a median follow-up of 3.5 years (IQR 1–7) and 79 313 echocardiograms, 11 646 (40%) patients experienced the primary outcome. Significant TR was independently associated with worse outcomes [adjusted HR (aHR) 1.21, 95% CI 1.14–1.28,
Significant TR portends worse prognosis in HF. SGLT2i therapy is associated with improved outcomes and attenuated TR progression in this high-risk population, with findings limited by the observational design and potential residual confounding.
Contributors

Ranel Loutati
Author
Viana Copeland
Author
Shir Elimeleh
Author
David Hochstein
Author
Kobi Faierstein
Author
Assi Milwidsky
Author
Sagit Ben-Zekry
Author
Amit Segev
Author
Rafael Kuperstein
Author
Elad Maor
Author
You may be interested in