Intrinsic cardiac protection against arrhythmia in pulmonary arterial hypertension independent of hypoxia inducible factor 2-alpha activity
Cardiovascular Research


Abstract
Pulmonary Arterial Hypertension (PAH) is a debilitating condition whereby a rise in Pulmonary Vascular Resistance elevates pressure exerted on the right ventricle (RV), leading to cardiac remodelling that leads to right heart failure (RHF). RHF raises the risk for arrhythmia and mortality. Studies demonstrate that Hypoxia Inducible Factor 2-alpha (HIF2a), a transcription factor that regulates gene expression to adapt to a hypoxic environment, plays an important role in the development and progression of PAH.
This study aimed to elucidate the potential role of HIF2a on cardiac electrophysiological remodelling in chronic stages of PAH.
Male rats received a single dose of saline (CTR) or monocrotaline (MCT), an agent that induces PAH. At 2-weeks post-injection, rats commenced twice daily treatment with vehicle (VEH) or a HIF2a inhibitor (HIF2a-i). 4-weeks post-injection, end-point echocardiograms were conducted; hearts were then explanted and Langendorff perfused. Hearts underwent dynamic restitution pacing, during which action potentials were optically mapped. This was followed by Programmed Electrical Stimulation (PES) of the right ventricle. 2-way ANOVA; mean ± s.d. unless stated.
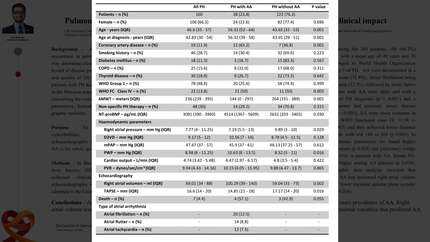
Echocardiographic Pulmonary Artery (PA) Acceleration Time to PA Ejection Time logarithmic ratios were significantly lower, indicative of higher PA pressures, in MCT VEH (-0.53 ± 0.11) and MCT HIF2a-i (-0.50 ± 0.07) than CTR VEH (-0.39 ± 0.03) and CTR HIF2a-i (-0.41 ± 0.06), respectively (p<0.05). Action Potential Duration (APD80) was significantly shorter in CTR HIF2a-i (79.11ms ± 14.83) than CTR VEH (93.99ms ± 11.08) and MCT HIF2a-i (105.3ms ± 12.37) (p<0.05). Heterogeneity indices of APD80 across the heart’s surface was significantly greater in CTR VEH (0.61 ± 0.18) and CTR HIF2a-i (0.53 ± 0.17) than MCT VEH (0.37 ± 0.11) and MCT HIF2a-i (0.38 ± 0.11), respectively (p<0.05), suggestive of higher risk for arrhythmia in non-diseased hearts. PES scores were significantly greater in CTR VEH (6.0, 3.0 – 6.0 IQR) and CTR HIF2a-i (5.0, 0.5 – 6.0 IQR) than MCT VEH (0.0, 0.0 – 1.0 IQR) and MCT HIF2a-i (0.0, 0.0 – 0.0 IQR), respectively (p<0.01), indicative of greater propensity for arrhythmias in CTR hearts than MCT diseased hearts.
Inhibition of HIF2a significantly shortens APD in healthy CTR hearts with no effect in MCT. In this study CTR hearts were found to be significantly more pro-arrhythmic and heterogenous for APD than MCT diseased hearts. This is suggestive of electrophysiological protection in MCT diseased hearts. It is hypothesised that the Langendorff perfusion rate was insufficient, thus producing a hypoxic environment, of which the MCT hearts had adapted to such conditions over 4 weeks, while the CTR hearts were unprepared for such hostilities. Further investigation is required to investigate this hypothesis and the conditions that elicit electrophysiological protection in MCT diseased hearts.
Contributors


Z Hua
Author
Y Shyam
Author
H A Prabhu
Author
V Kappadan
Author
E Zounis
Author
Z Habib
Author
C Brown
Author
Y Abdelghani
Author
E Zhang
Author
D Agha-Jaffar
Author
N S Peters
Author
Imperial College London London , United Kingdom of Great Britain & Northern Ireland

A Cowburn
Author
You may be interested in