6 to 12-month vs. 1-month dual antiplatelet therapy: comparative outcomes after aspirin cessation with HT supreme stent in the pooled PIONEER III and PIONEER IV trial analysis
European Heart Journal Supplements


Abstract
DAPT is crucial for preventing ischemic events following drug-eluting stents (DES) PCI, but increases bleeding risks. Randomised controlled trials (RCTs) showed that abbreviated DAPT could reduce bleeding without increasing ischemic risks. However, guidelines continue to recommend ≥6-month DAPT. The sirolimus release of the Healing Target SupremeTM DES (HT Supreme) is precisely timed to inhibit smooth muscle proliferation without excessive endothelium inhibition, showing clinical non-inferiority to XienceTM DES in the PIONEER III RCT with ≥6-month DAPT. The PIONEER IV RCT using 1-month DAPT offers data to compare outcomes under different DAPT regimens.
We pooled individual patient data of PIONEER III (NCT02607865, n=1051) and PIONEER IV (NCT0492319, n=1473), both are multicentre RCTs. PIONEER III included patients with CCS, unstable angina, or NSTEMI, who received de novo lesion PCI, excluding left main and CTO, while PIONEER IV included all-comer patients, including STEMI, and complex PCI. After PCI, PIONEER III patients received 6 or 12-month DAPT for CCS and ACS, respectively, while PIONEER IV patients received 1-month DAPT followed by ticagrelor monotherapy for 11 months. The primary endpoint was patient-oriented composite endpoint at 12 months (PoCE, composite of all-cause death, any myocardial infarction, and any revascularisation), adjudicated by independent clinical event committees. Major (Bleeding Academic Research Consortium, BARC 3 or 5) and clinically significant bleeding (BARC 2, 3, or 5) and the combination of PoCE and major bleeding (NACE) were assessed.
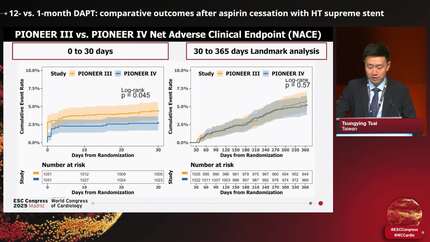
The baseline characteristics of HT-Supreme-treated patients were generally similar. However, hypertension and diabetes were more prevalent in PIONEER III. At 12 months, PoCE occurred in 86(8.2%) and 107(7.3%) PIONEER III and PIONEER IV patients, respectively, p=0.396. The incidence of Major bleeding was 1.4% and 2.1% in PIONEER III and PIONEER IV, p=0.215 while Clinically significant bleeding was similar at 2.8% vs. 2.7%, respectively, p=0.947. The incidence of NACE was 9.9% and 8.4% in PIONEER III and PIONEER IV, respectively, p=0.186. Landmark analysis after 30-day showed PoCE rate of 4.6% and 5.6% (figure) for PIONEER III and PIONEER IV, respectively. The incidence of bleeding was similar at both time points.
PCI with HT Supreme DES and 1-month DAPT demonstrated comparable PoCE and bleeding rates to longer DAPT without increased PoCE’s after aspirin cessation.
Contributors



L Rosseel
Author

N I C K Curzen
Author
University Hospital Southampton NHS Foundation Trust Southampton , United Kingdom of Great Britain & Northern Ireland
D Kereiakes
Author

A Baumbach
Author
St Bartholomews and Queen Mary University London , United Kingdom of Great Britain & Northern Ireland
S Windecker
Author
Y Hussian
Author
O Dressler
Author
A Lansky
Author
M Leon
Author


You may be interested in