Novel device success algorithm of the european association of percutaneous cardiovascular interventions (EAPCI) prospectively applied in the all-comer PIONEER IV trial
European Heart Journal Supplements


Abstract
Device success is a key endpoint for drug-eluting stents (DES) studies. However, inconsistent definitions have yielded varied success rates, hindering direct comparisons. We developed a device success algorithm with the European Association of Percutaneous Cardiovascular Interventions (EAPCI) to standardise adjudication, but it has not been prospectively applied in clinical trials with core lab adjudication.
In the PIONEER IV trial, we prospectively applied the EAPCI device success algorithm enriched by the core lab post-PCI angiography-derived fractional flow reserve (angio-FFR) to investigate the determining factors and prognostic implications of device success.
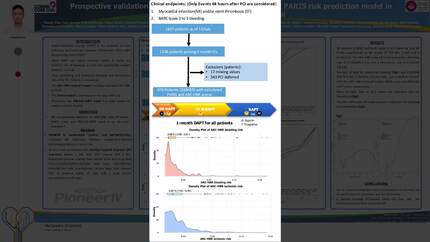
PIONEER IV (NCT04923191) is a multicenter, all-comers randomised controlled trial comparing PCI outcomes guided by angio-FFR versus usual care with unrestricted use of invasive physiology or intravascular imaging. The Healing-Targeted Supreme DES (HT Supreme) was used in both arms. An independent core lab (CORRIB core lab, Ireland) adjudicated device success following the EAPCI algorithm. This involved the implantation of the first assigned stent with post-PCI diameter stenosis <20%. New thresholds were enriched with post-PCI delta angio-FFR across the stent ≤0.05.
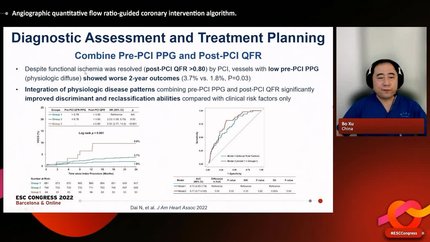
Among the first 1,270 patients in PIONEER IV, 1,090 lesions (QFR arm 557; usual-care arm 562) were targeted for treatment with the HT Supreme. Two lesions failed delivery and were treated medically or with a drug-coated balloon; 14 required crossover to a second HT Supreme or another DES due to deployment failure. Thus, 1,074 lesions were successfully implanted with the assigned stent. Site reports identified 41 lesions with residual stenosis exceeding the accepted threshold (visual/QCA residual stenosis <20%), resulting in an overall device success rate of 94.8%, success by arm was 94.8% (QFR) versus 95.6% (usual care), p = 0.651. After independent core-lab QCA adjudication, 101 lesions had residual stenosis ≥20%, reducing overall device success to 89.9%; success by arm was 90.5% (QFR) versus 87.0% (usual care), p = 0.081. Post-PCI Δangio-FFR ≤0.05 across the stent was achieved in 1,025/1,053 (97.3%). When applying the enriched device-success definition (core-lab QCA residual stenosis <20% and Δangio-FFR ≤0.05), success was 89.7% in the QFR arm (500 lesions) versus 84.0% in the usual-care arm (472 lesions), p = 0.006.
Operator-reported device success with HT Supreme was high (94.8%), but core-lab QCA adjudication yielded a lower rate (89.9%), indicating underestimation of residual stenosis by operators. Core-lab QCA should be considered essential for unbiased DES performance assessment. Moreover, when device success incorporated post-PCI Δangio-FFR, QFR guidance achieved higher success than usual care, supporting routine integration of physiology into PCI workflow.
Contributors


A Oshima
Author
J Wykrzykowska
Author
L Rosseel
Author

N Curzen
Author
University Hospital Southampton NHS Foundation Trust Southampton , United Kingdom of Great Britain & Northern Ireland
V Flore
Author
Y Bataille
Author
M Pankert
Author
C Von Birgelen
Author
K De Wilder
Author


You may be interested in