PO97
Predicaments in diagnosing victim of sudden cardiac arrest in an adolescent
European Journal of Preventive Cardiology


Abstract
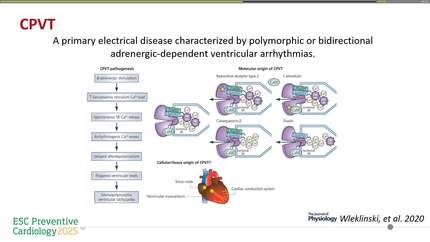
Sudden cardiac arrest in a young person is always a devastating experience for the patient’s family. Catecholaminergic Polymorphic Ventricular Tachycardia (CPVT) is a rare form of inherited arrhythmia syndrome that can lead to polymorphic ventricular arrhythmia triggered by physical or emotional stress. Most cases of CPVT are due to pathogenic gain-of-function mutations in the gene encoding the cardiac ryanodine receptor calcium channel (RYR2). Due to the high polymorphism of RYR2, interpreting novel variants is very challenging.
We present a 14-year-old male who suffered out-of-hospital cardiac arrest while helping his family with field work and driving a tractor. Resuscitation was initiated by witnesses and then continued by paramedics. Ventricular fibrillation (VF) was confirmed, and two shocks were delivered, restoring sinus rhythm. The patient was transported by air to our institution and admitted to the intensive care unit (ICU). After admission, he stabilized; his ECG showed transient post-ischemic changes that normalized over a few days.
While in the ICU, the patient experienced a short episode of polymorphic VT that quickly deteriorated into VF (Fig. 1), successfully treated with defibrillation. In diagnostic workup, his ECG did not show QT prolongation or Brugada pattern in normal and high RV leads. Extended ECG monitoring revealed no ventricular ectopy. Echocardiography initially showed impaired ejection fraction, which normalized later, and no evidence of structural changes or cardiomyopathy. A CT scan demonstrated normal coronary artery anatomy.
Extended history revealed that the patient had experienced a syncope during field work a few weeks earlier but recovered spontaneously and did not seek medical advice. Family history was negative for sudden cardiac death or syncope. The patient’s hemodynamic status gradually improved, allowing weaning from ventilator and inotropic support. However, he suffered severe hypoxic brain injury, and due to his neurological status, exercise testing was not feasible. Genetic sequencing revealed a rare RYR2 variant (c.12370A>G).
Inherited arrhythmia was suspected early, with CPVT considered likely. Although clinical features were atypical—VF on two occasions rather than recurrent syncope or bidirectional VT—the genetic finding supported this diagnosis. The identified RYR2 variant, previously reported in CPVT and classified as likely pathogenic, strengthened the case. The patient was treated with propranolol and flecainide, with no further arrhythmic events. His immediate family was referred for cardiac evaluation and genetic counselling.
This case illustrates the diagnostic challenges of CPVT, where genetic data may guide interpretation when clinical presentation does not fully match the classic profile.
Contributors

Tomasz Ksiazczyk
Author
Radoslaw Pietrzak
Author
Izabela Pągowska-Klimek
Author
Magdalena Mierzewska-Schimdt
Author
Dorota Czapczak
Author
Karolina Skubisz
Author
Klaudia Obsznajczyk
Author
Bozena Werner
Author
You may be interested in