Intracardiac echocardiography guided anatomical approach to cardioneuroablation: feasibility and outcomes
EP Europace Journal


Abstract
Anatomical studies have documented a close topographical relationship between the ganglionated plexi (GP) containing parasympathetic inputs to the sinus node (SN) and atrioventricular node (AVN) and the epicardial fat pads (FPs) within the Waterston’s interatrial groove. We aimed to investigate the feasibility and outcomes of a novel anatomical approach to cardioneuroablation (CNA) that targets the atrial areas adjacent to the interatrial FPs identified with intracardiac echocardiography (ICE).
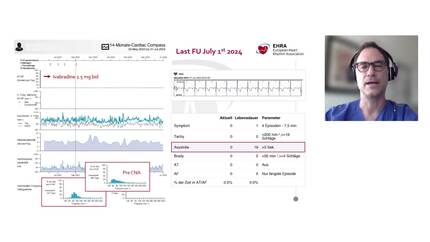
About 17 patients [37.3 ± 10.2 years, 47% female] undergoing CNA for recurrent vasovagal syncope and documented sinus pauses (
An ICE-guided anatomical approach to CNA targeting visible FPs at the Waterston’s groove is a feasible and effective strategy to achieve SN/AVN vagal denervation, with good outcomes at mid-term follow-up.
Contributors

Medhat Farwati
Author
Ayman A Hussein
Author

William Bautista
Author
Koji Higuchi
Author
Bryan Baranowski
Author
Mandeep Bhargava
Author
Thomas D Callahan
Author
Mina K Chung
Author
Roy Chung
Author
Arwa Younis
Author
Jeffery Courson
Author
Thomas J Dresing
Author
Mohamed Kanj
Author
Arshneel Kochar
Author
Robert Koeth
Author
Justin Z Lee
Author
Ioan Liuba
Author
David O Martin
Author
Kenneth Mayuga
Author
Shady Nakhla
Author
John Rickard
Author
Walid I Saliba
Author
Jakub Sroubek
Author
Tyler L Taigen
Author
Niraj Varma
Author
James Witten
Author
Edward Soltesz
Author
Carlos Tapias
Author
Luis Saenz
Author
Oussama Wazni
Author
Pasquale Santangeli
Author