Shortest pulmonary vein atrial fibrillation cycle length identifies pulmonary vein isolation responders beyond clinical atrial fibrillation pattern: the FARS-AF II study
EP Europace Journal


Abstract
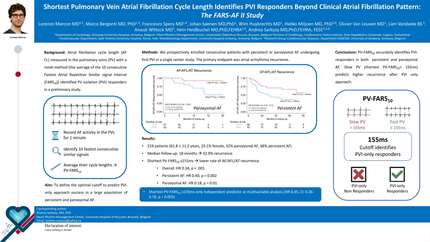
Atrial fibrillation cycle length (AF-CL) measured in the pulmonary veins (PVs) with a novel simple method [the average of the 10 consecutive Fastest Atrial Repetitive Similar signal interval (FARS10)] accurately identified pulmonary vein isolation (PVI) responders in a preliminary study. This study aims to evaluate differences in PV-FARS10 between paroxysmal and persistent AF and to define the optimal cut-off to predict PVI-only approach success in a large population.
We prospectively enrolled consecutive patients with persistent or paroxysmal AF undergoing first PVI in a single-centre study. The primary endpoint was atrial arrhythmia recurrence. A total of 219 patients (61.8 ± 11.2 years, 25.1% female) were included, with 70 patients (32%) having paroxysmal AF and 149 patients (68%) persistent AF. After a median follow-up of 18.0 [interquartile range (IQR) 10.2–42.3] months, 72 (32.9%) patients experienced AF/atrial flutter (AFL)/atrial tachycardia (AT) recurrence. Patients with shortest PV-FARS10 ≤ 155 ms had a lower rate of AF/AFL/AT recurrence compared to those with shortest PV-FARS10 > 155 ms in the overall population (HR 0.34,
PV-FARS10 can accurately identify PVI responders among patients with persistent and paroxysmal AF. Patients with slow PV (shortest PV-FARS10 > 155 ms) experience a higher rate of AF/AFL/AT recurrence after PVI-only approach. The shortest PV-FARS10 ≤ 155 ms occurs more frequently in paroxysmal AF patients than in persistent AF patients.
Contributors



Francesco Spera
Author

Wim Huybrechts
Author
Hielko Miljoen
Author
Lien Vandaele
Author
Anouk Wittock
Author


You may be interested in