Early assessment of atrial dysfunction severity using an AI-powered FCN from baseline echocardiography
European Heart Journal - Digital Health


Abstract
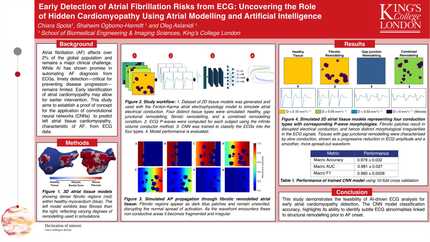
Accurately stratifying the severity of atrial dysfunction (AF) at a patient’s initial presentation represents a complex yet indispensable challenge.
We aimed to train and validate a fully connected network (FCN) on tabular data—comprising feature columns and a ground-truth label column—to achieve robust binary classification of severe versus non severe atrial dysfunction.
We prospectively evaluated 225 patients hospitalized for AF during 2 years of follow up. A binary ground-truth label indicating severe or non-severe atrial dysfunction was assigned to each patient, defined based on cardiac rhythm at 2 years of follow up. After initial cleaning, missing values were imputed via forward-fill (i.e., each missing entry replaced by the most recent available observation) yielding 359 features across 250 patients. We then stratified by label and split the data 80/20 into training and validation sets. Continuous features were standardized using the mean and standard deviation; binary features were left unchanged. The prepared data were loaded in batches of 32 for model training. Our FCN Binary Classifier comprised three fully connected hidden layers (128 → 64 → 32 units), each followed by ReLU activation and 20% dropout, and a final linear output neuron. We optimized the network using Binary Cross-Entropy with Logits Loss and the Adam optimizer (learning rate 1 × 10−5), with gradient clipping (max-norm 1.0) and early stopping (patience = 50 epochs) over a maximum of 100 epochs. To assess generalizability, we performed five-fold stratified cross-validation (batch size 32, learning rate 1 × 10−5), reporting accuracy, precision, recall, F1-score, and confusion matrices. For interpretability, we ranked feature importance by computing the empirical covariance of input gradients and conducting permutation-based importance analysis, thereby identifying the variables most influential to the model’s predictions.
On the held-out validation set, the FCN achieved an accuracy of 88.0%, with a precision of 71.43%, recall of 83.33%, and an F1 score of 76.0% (Figure 1). The confusion matrix comprised 34 true negatives, 4 true positives, 2 false positives, and 10 false negatives, demonstrating balanced performance across both classes. These metrics are expected to improve further through the iterative feedback and correction cycles described in the Methods. The most influential features in echocardiography associated with atrial dysfunction are displayed in Figure 2.
Our FCN-based approach demonstrated strong performance in classifying severe versus non-severe atrial dysfunction, defined based on cardiac rhythm at M24, achieving an 88.0% accuracy and balanced precision–recall metrics on an independent validation set. The integration of empirical covariance analyses provided transparent insights into feature importance, facilitating clinician engagement through iterative feedback cycles.
Contributors



A Cohen
Author
J Reisberg
Author
E Patte
Author
E Sotto
Author
P Le Bos
Author
L Benoudiba-Campanini
Author
A Newson
Author

You may be interested in