Bleeding risk using non-steroidal anti-inflammatory drugs in anticoagulated patients with atrial fibrillation: a nationwide cohort study
European Heart Journal - Quality of Care and Clinical Outcomes


Abstract
Limited data exist on the bleeding risk associated with concomitant use of non-steroidal anti-inflammatory drugs (NSAIDs) and individual direct oral anticoagulants. We investigated the bleeding risks of NSAID use in patients with atrial fibrillation (AF) who were receiving all available oral anticoagulants.
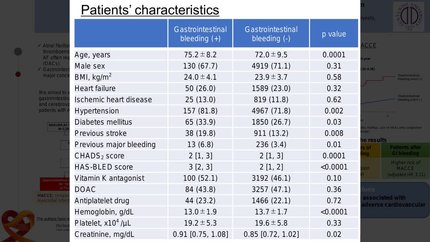
This nationwide cohort study included 114 119 patients with first-time diagnosed AF who initiated oral anticoagulation during 2012-22. Time-dependent multivariate cause-specific Cox regression assessed the association between NSAID use and hospital-diagnosed bleeding episodes, calculating adjusted hazard ratios (aHRs). Rates of hospital-diagnosed bleeding events per 100 person-years were 6.2 with NSAID use vs. 3.9 without (number needed to harm = 43 patients treated for 1 year). Compared with non-use, NSAID use was associated with increased rates of hospital-diagnosed bleeding overall [aHR, 1.81; 95% confidence interval (CI), 1.59-2.06], gastrointestinal bleeding (aHR, 2.30; 95% CI, 1.92-2.76), thoracic/respiratory tract bleeding (aHR, 1.59; 95% CI, 1.13-2.24), urinary tract bleeding (aHR, 1.48; 95% CI, 1.17-1.88), and anaemia caused by bleeding (aHR, 3.50; 95% CI, 2.33-5.26). NSAID use increased bleeding rates across all anticoagulants: rivaroxaban (aHR, 2.05; 95% CI, 1.64-2.57), apixaban (aHR, 2.15; 95% CI, 1.70-2.72), dabigatran (aHR, 1.40; 95% CI, 0.92-2.13), edoxaban (aHR, 2.87; 95% CI, 1.26-6.53), and warfarin (aHR, 1.46; 95% CI, 1.07-1.98). Results were consistent across NSAID subtypes.
NSAID use was associated with a nearly two-fold increase in hospital-diagnosed bleeding among patients with AF receiving oral anticoagulation. The risk appeared highest with edoxaban, followed by apixaban and rivaroxaban, and lowest with dabigatran and warfarin. The risk was not restricted to the gastrointestinal tract.
Contributors


You may be interested in