Dose titration among patients receiving vericiguat in real-world clinical practice and association with clinical outcomes and health care resource use
European Heart Journal


Abstract
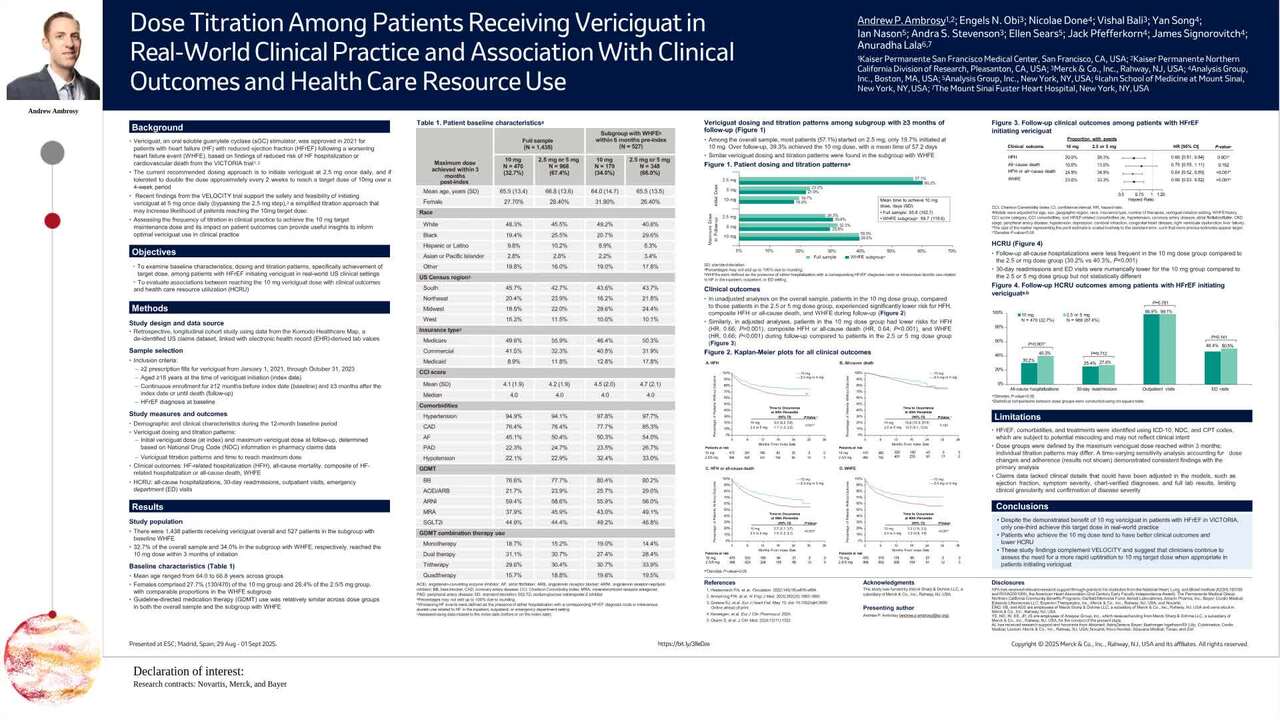
Vericiguat is indicated to reduce cardiovascular (CV) death and heart failure (HF) hospitalization risk in adults with symptomatic HF with reduced ejection fraction (HFrEF) following a worsening HF event (WHFE), based on the VICTORIA trial, where most patients received the target daily dose of 10 mg. The frequency of titration to 10 mg in clinical practice and its impact on outcomes is unclear.
This study examines baseline characteristics, dosing and titration patterns, specifically achievement of target dose, and association of dose with clinical outcomes and health care resource use (HCRU) among patients initiating vericiguat in real-world U.S. clinical settings.
Adult US patients with HFrEF and ≥2 vericiguat fills between (01/01/2021-10/31/2023) were identified using claims from the Komodo Research Database. The first vericiguat prescription was defined as index date. Patients were required to have continuous health plan enrolment for ≥12 months pre-index (baseline) and ≥3 months post-index or until death (follow-up). Baseline characteristics were assessed, stratified by maximum dose achieved within 3 months post-index (i.e., 10 mg or 2.5 mg/5 mg), including in a subgroup with WHFE in the 6 months pre-index. Initial vericiguat dose and titration patterns were also assessed. Clinical outcomes and HCRU were evaluated during follow-up in the overall cohort. Cox proportional hazards models, adjusted for patient and treatment characteristics, were used to assess clinical outcomes.
Among 1,438 patients overall and 527 in the subgroup with WHFE in the 6 months pre-index, only 470 (32.7%) and 179 (34.0%), respectively, achieved a 10 mg dose within 3 months of initiation. Baseline characteristics, including guideline-directed medical therapy use, as well as vericiguat initiation and titration patterns, were similar in the overall cohort vs. the WHFE subgroup (Table 1). In adjusted analyses, patients in the 10 mg dose group had lower risks of HF-related hospitalizations (HFH) (HR: 0.66; 95% CI: 0.51–0.84; p=0.001), WHFE (HR: 0.66; 95% CI: 0.53–0.82; p<0.001), and composite HFH or all-cause death (HR: 0.64; 95% CI: 0.52–0.80; p<0.001) during follow-up compared to patients in the 2.5 or 5 mg dose group (Table 2). Additionally, patients in the 10 mg dose group were less likely to experience all-cause hospitalizations during follow-up compared to patients in the 2.5 or 5 mg dose group. Proportions of patients with readmissions, outpatient visits, and emergency department visits were similar between the two groups.
Despite the demonstrated benefit of 10 mg vericiguat in patients with HFrEF in VICTORIA, only one-third achieve this dose in real-world practice. Patients who achieve the 10 mg dose tend to have better clinical outcomes and lower HCRU. Clinicians should continue to assess the need for uptitration to 10 mg when appropriate in patients initiating vericiguat.
Contributors

A P Ambrosy
Author
E N Obi
Author
Y Song
Author
I Nason
Author
J Pfefferkorn
Author
E Sears
Author
J Signorovitch
Author
You may be interested in