Guideline-directed medication therapy use among patients with HFrEF receiving vericiguat: comparing findings from a real-world study to clinical trials
European Heart Journal


Abstract
Despite the advent of guideline directed medical therapy (GDMT) for heart failure with reduced ejection fraction (HFrEF), residual risk for morbidity and mortality is significant. Vericiguat was approved in 2021 by the FDA for adults with symptomatic HFrEF and a recent worsening heart failure event (WHFE) based on the VICTORIA trial, to improve outcomes. The ongoing VICTOR trial is evaluating its use in patients without recent WHFE. How characteristics and GDMT use in real-world vericiguat initiators compare to trial participants is unclear.
This retrospective study aimed to describe baseline GDMT use in patients initiating vericiguat in real-world settings in comparison to the VICTOR and VICTORIA trials.
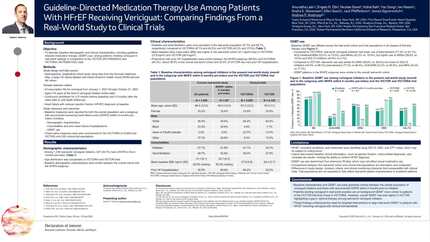
Using the Komodo Research Database (01/01/2020–10/31/2023), we evaluated US adults with HFrEF and ≥2 vericiguat fills. Index date was the first vericiguat fill. Patients were required to have HFrEF diagnosis during the 12-month baseline and continuous baseline health plan enrolment for ≥3 months post-index or until death. Baseline GDMT use and key demographic and clinical characteristics were assessed among all patients with HFrEF initiating vericiguat, including a subgroup with documented WHFE in the 6 months pre-index. Findings were compared to patients enrolled in the VICTOR (n=6,105) and VICTORIA (n=5,050) trials for vericiguat.
Among 1,438 real-world vericiguat initiators, 527 had WHFE in the 6 months pre-index (Table 1). Baseline characteristics and GDMT use were similar between the overall cohort and the WHFE subgroup. Age distribution was comparable to VICTORIA and VICTOR, but racial composition differed, with a higher proportion of Black patients in the real-world cohort (23.5% vs. 4.9% [VICTORIA] vs. 7.7% [VICTOR]), reflecting the high prevalence of Black patients in the U.S. HF population. Baseline GDMT use varied between the real-world cohort and trial populations in all classes of first line therapy. Compared to VICTORIA, real-world vericiguat initiators had lower use of beta-blockers (77.3% vs. 93.1%), ACE inhibitors/ARBs (23.2% vs. 73.5%), and MRAs (43.3% vs. 70.4%) but higher use of ARNI (58.8% vs. 14.5%) and SGLT2 inhibitors (44.6% vs. 3.1%). GDMT use in the real-world cohort more closely resembled VICTOR than VICTORIA, particularly for ARNI (58.8% vs. 56.0%) and SGLT2 inhibitors (44.6% vs. 59.1%). However, beta-blocker (77.3% vs. 94.4%), ACE inhibitor/ARB (23.2% vs. 38.3%), and MRA (43.3% vs. 77.7%) use remained lower.
Patients initiating vericiguat in real-world clinical practice have background GDMT use more similar to those in VICTOR than in VICTORIA. However, VICTOR patients were overall better treated than real-world vericiguat initiators, highlighting a gap in optimal GDMT implementation. These findings underscore the need for targeted interventions to align real-world treatment with clinical trial standards.
Contributors

E N Obi
Author
Y Song
Author
I Nason
Author
E Sears
Author
J Pfefferkorn
Author
J Signorovitch
Author
A P Ambrosy
Author
You may be interested in