Sympathetic vasoconstrictor constraint on exercise capacity in heart failure: does biological sex matter?
European Heart Journal


Abstract
Exercise intolerance in heart failure (HF) predicts both quality of life and survival. Female patients often present with more disabling symptoms. We discovered, in HF, regardless of left ventricular ejection fraction (LVEF), a ‘paradoxical’ reflex increase in vasoconstrictive muscle sympathetic nerve activity (MSNA) during 1-leg cycling exercise in patients across the spectrum, absent in healthy individuals, and an inverse relationship between MSNA during cycling and exercise capacity (peak oxygen uptake; V̇O2peak). Purpose Our present aim was to test the hypothesis that females with HF display a greater ‘paradoxical’ muscle sympatho-excitatory response than males.
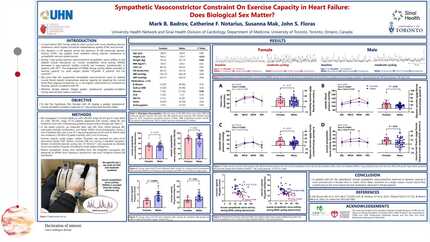
We investigated 15 female (68±8 yrs; LVEF: 40±16%, range 20-67; BMI: 30±9 kg/m2) and 41 male (64±9 yrs; LVEF: 38±15%, range 15-73; BMI: 29±5 kg/m2) patients with chronic, stable HF, treated for such with contemporary guideline-based medical therapy. In the seated position, we measured heart rate (HR), blood pressure (BP), and MSNA (microneurography) during 2 minutes of baseline rest and 4 minutes of 1-leg cycling (2 minutes each at mild [0 load] and moderate [~30-40% V̇O2peak] intensity). V̇O2peak was obtained by open circuit spirometry during a standard, symptom-limited incremental cycling test (15 W·min-1).
Resting HR (64±10 vs. 63±10 beats·min-1; P=0.89), systolic BP (115±19 vs. 105±16 mmHg; P=0.09), and diastolic BP (65±12 vs. 64±10 mmHg; P=0.84) did not differ between females and males, respectively. Resting MSNA also was not different between females and males (51±11 vs. 50±11 bursts·min-1; P=0.70), whereas V̇O2peak was lower in females (15±5 vs. 21±8 ml·kg-1·min-1; P<0.01). During 1-leg cycling exercise, HR (+12±6 vs. +10±6 beats·min-1 at moderate cycling) and diastolic BP (+13±10 vs. +7±8 beats·min-1 at moderate cycling) increased similarly in females and males, respectively (both P>0.05), whereas the systolic BP response during moderate cycling was greater in females (+25±22 vs. +15±9 mmHg; P=0.03). Similarly, compared to baseline rest, MSNA increased during mild and moderate cycling in both sexes (all P<0.05), yet the magnitude of response during moderate cycling was greater in females than males (+9±6 vs. +4±10 bursts·min-1; P=0.03). In both sexes, the level of MSNA during moderate intensity cycling related inversely to V̇O2peak, explaining 42% of the variance in females (P<0.01), yet only 10% in males (P=0.05).
In patients with HF, the ‘paradoxical’ muscle sympathetic vasoconstrictor response to dynamic exercise is more pronounced in females than in males, which likely constrains to a larger extent, skeletal muscle blood flow and increases resistance, thereby contributing to the more severe exercise intolerance observed in female patients. Our findings may help inform novel, female-specific therapeutic strategies designed to reverse such sympathetic disturbances, alleviate symptoms, and improve exercise capacity.
Contributors


You may be interested in