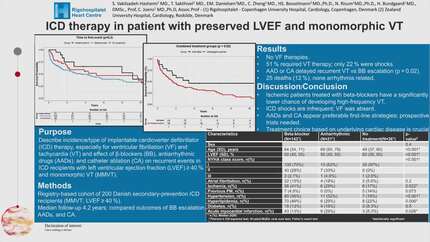
ICD therapy in patients with preserved LVEF and monomorphic VT
European Heart Journal


Abstract
Several meta-analyses have questioned if an ICD improves prognosis and quality of life in patients with preserved ejection fraction who receives an ICD for monomorphic ventricular tachycardia (VT), and if alternative treatments such as anti-arrhythmic drugs (AAD)´s or catheter ablation (CA) should be considered as first line therapy.
To describe the type and incidence of ICD therapy, particularly the incidence of future ICD therapy for ventricular fibrillation (VF) and VT as well as the effect of beta blocker (BB), AAD, and CA on repeated ICD therapy observed in secondary prevention ICD recipients with preserved LVEF and monomorphic ventricular tachycardia (MMVT).
A registry-based cohort study using data from electronic patient files and the Danish Pacemaker and ICD Registry (DPIR). Eligible patients had LVEF ≥ 40% and an ICD implanted for secondary prevention due to MMVT. Patients with prior cardiac arrest or VF were excluded. VT episodes and corresponding ICD therapies were reviewed, and treatment modifications were analyzed including treatment with BBs, AADs and CA.
A total of 200 patients were enrolled (67 ischemic (IHD), 78 non-ischemic (non-IHD), and 52 without known cardiac disease). Non-IHD patients younger (67 yr vs 59 vs 56 yr p=<0.001).
There was no significant difference in symptom presentation at baseline (presyncope/syncope 66.7% vs. 51.2% vs 60.4% p=0.50). The baseline VT cycle length was lowest in the IHD group (197bpm vs 212 bpm vs 218 bpm p=0.0072). None of the 200 patients received therapy for VF during a median follow-up of 4.2 years [IQR 2.0-14.1]. 102 patients (51%) received therapy for at least one new VT episode and 71 (35.5%) for ≥ 2.
Among 261 therapies for VT episodes 57 (21.8%) were shock therapy in 51 patients.
There was no significant difference in time to next VT event between untreated patients and patients treated with BB´s or AADs (p = 0.2), but for the second event, AAD and CA showed significantly better effects than patients increased in BB or unchanged treatment (p = 0.02) (figure 1 and figure 2). A total of 25 out of 200 patients died, none of the deaths were cardiac or arrhythmia related.
The findings of this study challenge the current paradigm of ICD use for secondary prevention in patients with preserved LVEF and MMVT. Despite a high incidence of recurrent VT episodes, none of the patients experienced VF and ICD shocks were infrequent. CA and AADs reduced the risk of recurrent VT episodes suggesting their potential role as alternative treatment strategies in this group. The absence of arrhythmic-related deaths further supports these findings. These results highlight the need for future prospective trials in this area particularly involving CA. Time to first event based on treatments Time to second event based on treatment
Contributors



You may be interested in