Timing of first-time catheter ablation in patients with atrial fibrillation and heart failure - Insights from a Danish nationwide cohort
European Heart Journal


Abstract
Atrial fibrillation (AF) patients with heart failure (HF) face elevated risks of AF recurrence and major adverse cardiovascular events (MACE). Catheter ablation (CA) of AF for rhythm control is an established treatment, but a (time-dependent) progressive atrial and ventricular remodelling and fibrosis may limit the efficacy. A reduction in the diagnosis-to-ablation-time (DAT) could potentially play a crucial role in outcomes.
To examine the influence of DAT on AF recurrence and MACE in patients with AF and HF.
This nationwide cohort study utilized real-world data from Danish healthcare registries. Patients over 18 with a diagnosis of both AF and HF who underwent first-time CA from January 1st, 2010, to December 31st, 2020, were identified, with inclusion set on the date of ablation. Exposure of interest was timing of the ablation by DAT, categorizing patients into early (<1 year after AF diagnosis), intermediate (1-3 years after AF diagnosis) and late (>3 years after AF diagnosis) ablation groups. Primary endpoint included AF recurrence, after a 3-months blanking period, and MACE. AF recurrence was defined as first occurrence of either AF hospitalization, new prescription of anti-arrhythmic drugs (class 1C anti-arrhythmic drugs, dronedarone or amiodarone), electrical cardio-version, or AF re-ablation, with death as competing risk and censoring for emigration. MACE included hospitalization for HF, stroke, acute myocardial infarction, and death. Two-year cumulative incidences were reported for AF recurrences and MACE. The relative risk of recurrent AF and MACE by DAT were examined by Cox proportional hazard models with the early group as the reference.
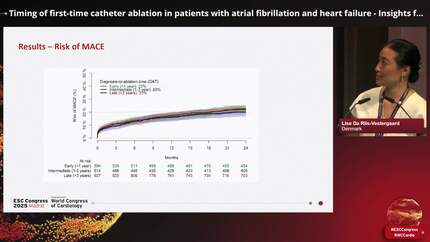
This study included 2,035 patients with AF and HF: 594 in the early group, 514 in the intermediate, and 927 in the late group. Median age increased by DAT group (61, 63, and 65 years). Most patients were male (80%, 76% and 77%) and had persistent AF (68%, 58%, 58%). The two-year absolute risk of AF recurrence increased by DAT group: 41% (early), 54% (intermediate) and 64% (late) (Figure 1). The adjusted analysis revealed a 25% higher risk in the intermediate group (HR: 1.25, 95% CI: 1.04-1.51), and 49% higher risk in the late group (HR: 1.49, 95% CI: 1.26-1.75) compared to the early group (Figure 2). The absolute risk of MACE remained stable at 22%, 20% and 22% (Figure 1). The adjusted analysis confirmed no statistically significant difference, with HRs of 0.93 (95% CI: 0.70-1.24) and 1.05 (95% CI: 0.82-1.35) for the intermediate and late group, respectively (Figure 2).
The timing of ablation for patients with AF and HF may impact catheter ablation efficacy. Longer DAT was associated with increased risk of AF recurrence, but there was no significant increased risk of MACE. Cumulative incidences Cox proportional hazards analysis
Contributors

L I S E Riis-Vestergaard
Author
Rigshospitalet - Copenhagen University Hospital Copenhagen , Denmark

C A S P E R Binding
Author
G U N N A R Gislason
Author
You may be interested in