Competing risks of ischemic stroke, intracranial bleeding, and mortality in patients with atrial fibrillation and prior intracranial hemorrhage without an anticoagulation regimen
European Heart Journal


Abstract
A history of intracranial hemorrhage (ICH) is a significant risk factor for bleeding complications but also increases the risk of ischemic stroke (IS). Therefore ICH creates a clinical dilemma in patients with an incident atrial fibrillation (AF) and need of oral anticoagulation (OAC). The patient's overall risk factor burden is crucial in this decision-making process.
We aimed to assess the competing risks of recurrent ICH, IS, and death from other causes (mortality) in AF patients who refrained from OAC. Absolute risk estimates were calculated using the cumulative incidence function, considering cerebrovascular events and mortality as competing risks.
We linked data from nationwide Finnish administrative registries to establish a comprehensive population-based database of patients with incident AF between 2008-2018. In this sub study, patients were included if they had AF diagnosed between 2010-2018, had a history of ICH at least 120 days before AF diagnosis and did not purchase any OAC during the two-year follow-up. Competing absolute risks and cumulative incidences of ICH, IS, and mortality were estimated and stratified by CHA₂DS₂-VA score categories.
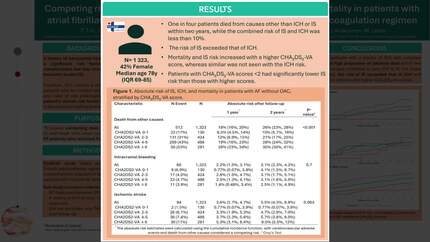
The cohort included 1,323 patients (42% female, median age 78 years [IQR 69–85]). Overall, one in four patients died from causes other than ICH or IS within two years, while the combined risk of IS and ICH was less than 10%. The risk of IS exceeded that of ICH. Mortality and IS risk increased with a higher CHA₂DS₂-VA score, whereas similar was not seen with the ICH risk. Patients with CHA₂DS₂-VA scores <2 had significantly lower IS risk than those with higher scores.
Among AF patients with a history of ICH who refrained from OAC, a high proportion of patients died within two years from causes unrelated to new ICH or IS. For those who survived, the risk of IS exceeded that of ICH and was higher in patients with higher CHA₂DS₂-VA scores.
Figure 1. absolute risk of ischemic stroke, intracranial bleeding, and mortality in patients with AF without OAC, stratified by CHA₂DS₂-VA score.
Figure 2. Cumulative incidence of ischemic stroke, intracranial bleeding, and mortality in patients with AF and without OAC stratified by CHA₂DS₂-VA score.
Contributors

J Putaala
Author

J Haukka
Author
M Linna
Author
J Kinnunen
Author
A Aro
Author
P Mustonen
Author

M Lehto
Author
You may be interested in