Left ventricular remodeling index to predict ventricular tachyarrhythmia in dilated cardiomyopathy with ejection fraction <35%
European Heart Journal


Abstract
Myocardial fibrosis assessed by cardiac magnetic resonance (CMR) with late gadolinium enhancement (LGE) imaging has emerged as a powerful predictor for sudden cardiac death (SCD) in dilated cardiomyopathy (DCM). However, in the cohort of DCM patients with LVEF <35%, isolated LGE may not exhibit significant difference between those with and without adverse outcomes. In such circumstances, morphological parameters may provide additional prognostic value for DCM patients with left ventricular ejection fraction (LVEF) <35%. The predictive value of LV remodeling index (LVRI), a novel geometry parameter derived from CMR, for ventricular tachyarrhythmia (VTA) in this population remains unclear.
To explore the predictive value of LVRI for VTA in patients with nonischemic DCM with LVEF <35%.
In this retrospective single-center study, consecutive DCM patients with LVEF <35% (n=271) who underwent CMR imaging were followed up. The study endpoint was VTA, a composite of sudden cardiac death or major ventricular arrhythmias. The newly derived LVRI was defined as the cubic root of the LV end-diastolic volume divided by the maximal LV wall thickness. Competing risk regression analysis and Kaplan-Meier analysis were used to evaluate the association of LVRI with VTA.
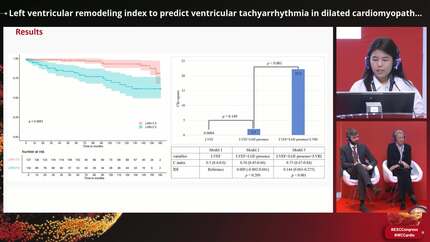
During a median follow-up of 71 months (interquartile range: 17–134 months), 35 (12.9%, mean age 46.7 years, 27 males) participants reached VTA events. The presence of late gadolinium enhancement (LGE) (62.9% vs. 60.2%, p = .761) and LVEF (23.3±6 vs. 21.9±10.3, p = .197) were not significantly different between the patients with and without endpoint. Kaplan-Meier curve analysis showed that participants with LVRI ≥7.5 were more likely to experience VTA (p < .0001). In the multiple competing risk analysis, when heart transplantation and heart failure (HF)-related death were counted as competing risks, LVRI ≥7.5 (HR, 2.496; 95% CI: 1.213-5.138; p = .013) was observed as an independent predictor of VTA after adjusting for age, sex and left bundle branch block.
For patients with nonischemic DCM with LVEF <35%, CMR-assessed LVRI ≥7.5 was associated with lethal VTA events. Central Illustration
Contributors

X I Jia
Author
State Key Laboratory of Cardiovascular Disease, Fuwai Hospital, National Center for Cardiovascular D Beijing , China
S H I H U A Zhao
Author
State Key Laboratory of Cardiovascular Disease, Fuwai Hospital, National Center for Cardiovascular D Beijing , China
You may be interested in