Long-term prognostic implications of pericoronary inflammation assessed by pre-interventional computed tomography in patients with non-ST-segment elevation acute coronary syndrome
European Heart Journal


Abstract
Coronary computed tomography angiography (CCTA) could provide anatomical information instantly. Fat attenuation index (FAI) is derived from CCTA imaging and represents perivascular inflammatory status. Although a previous study reported the prognostic utility of pericoronary FAI in CCTA in patients with chronic coronary syndrome, the long-term prognostic impact of FAI before urgent coronary angiography in patients with non-ST-Segment elevation acute coronary syndrome (NSTE-ACS) remains unclear.
We investigated the association between baseline clinical characteristics and CCTA findings, including the average FAI of 3 coronary arteries (FAI-mean) derived from CCTA before urgent percutaneous coronary intervention (PCI) in patients with NSTE-ACS, and major adverse cardiac events (MACE) for long-term follow-up.
This retrospective study enrolled consecutive patients who underwent CCTA before urgent coronary angiography without known history of prior myocardial infarction or coronary revascularization. Patients who underwent unsuccessful PCI or who were lost to follow-up within 1 year after CCTA without any clinical events were excluded. MACE was defined as a composite of all-cause death and non-fatal myocardial infarction. We divided patients into 2 groups based on the occurrence of MACE and comparted clinical demographics and CCTA findings between the two groups.
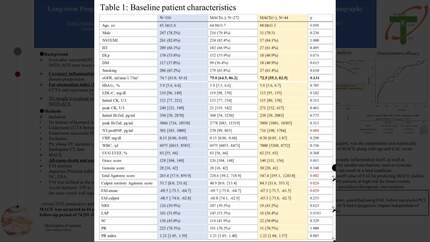
A total of 316 patients were included (247 (78.2%) men; 65.3±11.6 years old). MACE occurred in 44 (13.9%) patients during a median follow-up of 74 [51-107] months. A Multivariable Cox proportional hazards analysis showed that age, total calcium score, and FAI-mean were independently and significantly associated with MACE [hazard ratio; 1.04 (1.01-1.07), 1.00 (1.00-1.00) and 1.05 (1.00, 1.10), respectively. All p<0.05]. The receiver-operating characteristic (ROC) curve analysis showed that the best cut-off values of total calcium score and FAI-mean to predict MACE were 205 and -72.07 Hounsfield Unit (HU), respectively. The discriminant efficacy for predicting MACE was significantly improved when FAI-mean >72.07 HU was added to the reference clinical model; composite of age, male sex, hypertension, left ventricular ejection fraction and total calcium score >205 (c-statistics: 0.662 vs 0.711, p=0.028).
Pericoronary inflammation before successful PCI in patients with NSTE-ACS had a prognostic impact independent of conventional risk factors.