Planimetry in aortic valve stenosis using computed tomography angiography - bicuspid cut-off determination
European Heart Journal


Abstract
Aortic valve (AV) stenosis is quantified by transthoracic echocardiography (TTE). However, stenosis severity can remain inconclusive when TTE severity parameters are incongruent. AV-area (AVA) by CTA-planimetry (pAVACTA) may aid in these cases.
Defining the role of CTA-planimetry for bicuspid (BC) AV stenosis by cut-off determination. TTE of conclusive patients with cut-off parameters established as Goldstandard for Tricuspid (TC) AVs was used as reference.
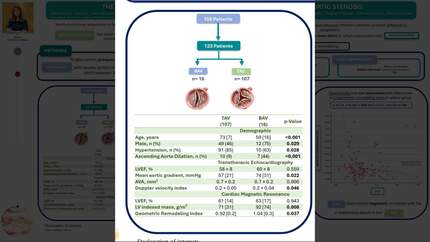
Severity classification of AV stenosis was performed using TTE with classification into conclusive if all three of the following criteria were congruent: Vmax≥4m/s & ∆Pm≥40mmHg & cAVATTE<1.0cm² (3+ "severe", 3- "non-severe"). Retrospective, single center screening of 4059 pre-TAVI-CTA-scans (2012- 2023) yielded 133 conclusive BC cases. Cut-off values for pAVACTA as a 4th severity criteria marker were determined by first correlating pAVACTA to cAVATTE directly and second comparing different pAVACTA values for predicting "severe" stenosis via receiver operator curve (ROC).
pAVACTA showed strong positive correlation with cAVATTE (Pearson-Correlation 0.780, p<0.001) with Linear Regression yielding a correlating factor (contraction coefficient CC) of 0.84 (95% CI [0.810, 0.861], p<0.001). ROC analysis (AUC 0.895, p<0.001) yielded a cut-off range with severe stenosis "likely" at pAVACTA≤1.08cm² (Sens. 88.3%, Spec. 77.3% via Youden’s index) and "unlikely" at ≥1.2cm2 (-LR 0.091 at <1.20cm²).
Having previously performed a similar analysis for TC Valves with resulting proposed pAVACTA cut-off values of ≤0.95cm² to support severe AS and ≥1.10cm2 to render it unlikely, direct comparison showed larger pAVACTA cut-off values for BC than TC Valves at a smaller CC (~0.84 vs ~0.91).
For a given pAVACTA the expected cAVATTE is smaller with this effect more pronounced in BC than in TC AVs. Cut-off values for pAVACTA as a 4th AV-stenosis severity marker should differentiate between BC and TC as hemodynamic impact depends on valve shape. Hemodynamic Effect of Valve Shape
Contributors

You may be interested in