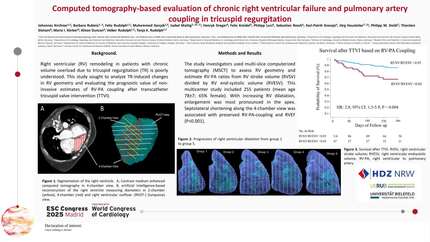
Computed tomography-based evaluation of chronic right ventricular failure and pulmonary artery coupling in tricuspid regurgitation
European Heart Journal


Abstract
Right ventricular (RV) remodeling and failure in patients with chronic volume overload due to tricuspid regurgitation (TR) is poorly understood. The right ventricular (RV)–pulmonary arterial (PA) coupling ratio has prognostic value in various conditions.
This study sought to analyze right ventricular (RV) geometry and the prognostic value of non-invasive estimates of RV-PA coupling and RV ejection fraction (RVEF) in tricuspid regurgitation after transcatheter tricuspid valve intervention (TTVI).
The study investigators used cardiac multi-slice computerized tomography (MSCT) to assess RV geometry and estimate RV-PA ratios from RV stroke volume (RVSV) divided by RV end-systolic volume (RVESV). MSCT-based RV-PA uncoupling was defined as a ratio <0.85 and reduced RVEF was defined as ≤45%. The primary endpoint was all-cause mortality at 1-year follow-up.
This multicenter study included 255 patients (mean age 78±7; 65% female). With increasing RV dilatation, enlargement of the diameter was most pronounced in the apical part of the ventricle (P<0.001). Basal- and mid-ventricular septolateral shortening was reduced in patients with impaired RVEF (P<0.001).
All-cause mortality occurred in 28 of 161 (17.4%) patients who underwent TTVI; 13 (11.4%) of whom had baseline RVSV/RVESV ratios greater than 0.85 and 15 (31.9%) had baseline RVSV/RVESV ratio <0.85 (HR: 2.8; 95% CI: 1.3-5.9; P = 0.004). Uni- and multivariable Cox Analyses revealed that MSCT-based RV-PA-coupling as well as RVEF were independently associated with higher risk for death.
The RV enlarges in chronic volume overload caused by tricuspid regurgitation especially at the RV apex. The loss of shortening in the basal and midventricular segments leads to a reduction in overall RVEF. Septolateral shortening of the RV plays a critical role in maintaining RV-PA coupling and RVEF, which are both independent and equal predictor of mortality following TTVI.
Contributors

M G Gercek
Author

H D Dreger
Author
F K Kreidel
Author
K P K Kresoja
Author
P L Lurz
Author

T G Gietzen
Author

T R Rudolph
Author
You may be interested in