Isolated tricuspid Libman–Sacks endocarditis in a patient with systemic lupus erythematosus and antiphospholipid syndrome: case report
European Heart Journal - Case Reports


Abstract
Libman–Sacks endocarditis (LSE) is an immune-mediated, culture-negative valvulopathy complicating systemic lupus erythematosus (SLE) and often amplified by antiphospholipid syndrome (APS). Although classically left-sided, isolated tricuspid involvement is rare. Advanced three-dimensional (3-D) quantification refines tricuspid regurgitation (TR) grading and informs surgical timing.
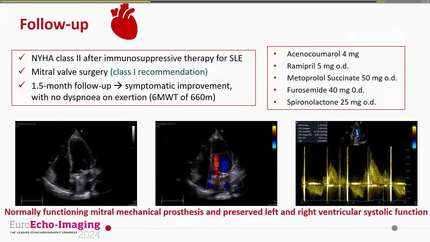
A 41-year-old woman with 2-year SLE and triple-positive secondary APS presented with 2 weeks of fever, migratory arthralgia, and a small non-traumatic subarachnoid haemorrhage (SAH). Serial blood cultures were negative. Transthoracic echocardiography showed multiple heterogeneous vegetations (largest 20 × 12 mm) on all tricuspid leaflets; 2-D PISA-EROA was 30 mm², while 3-D vena-contracta area (VCA) measured 0.95 cm², indicating massive TR. Cardiac computed tomography corroborated leaflet thickening and poor coaptation; transoesophageal echocardiography was deferred owing to recent SAH. A Heart Team favoured LSE over infective endocarditis. After high-dose corticosteroids for an SLE flare, surgery was deferred 21 days post-SAH and tricuspid valve replacement with a 31-mm bovine pericardial bioprosthesis was performed. Pathology confirmed sterile platelet–fibrin vegetations. Post-operatively, she received warfarin (target INR 2.5–3.5; heparin bridge), rituximab, hydroxychloroquine, and tapering prednisone. At 3 months, she was asymptomatic (NYHA I) with a competent prosthesis, normal right-sided dimensions, and improved lupus biomarkers.
This case highlights (i) the need to consider LSE in culture-negative right-sided endocarditis among SLE/APS patients; (ii) the clinical utility of 3-D VCA to reconcile discrepant 2-D measures and substantiate surgical indication; (iii) peri-operative strategies after recent SAH (timing and anticoagulation); and (iv) rationale for a bioprosthesis in the low-flow tricuspid position given thrombogenicity of mechanical valves, alongside lifelong vitamin K antagonist therapy mandated by APS. Early multimodality imaging, Heart Team decision-making, timely surgery, and optimized immunomodulation can yield excellent outcomes.
Contributors

Yancy Yuliana Erazo-Dorado
Author
Juan Carlos Rivera Guerrero
Author
Felipe Israel Lopez Trejo
Author
Rita Pavasini
Author
Andriana Anagnostopoulou
Author
Shahrukh Hashmani
Author
Deepti Ranganathan
Author
You may be interested in