Coronary artery bypass grafting with or without preoperative physiological stenosis assessment: a SWEDEHEART study
European Heart Journal


Abstract
Physiological flow assessment of coronary stenoses, such as fractional flow reserve, are routinely used to guide percutaneous coronary intervention, but it has not been equally recognized to guide coronary artery bypass grafting (CABG). Mid-term outcomes in CABG patients with and without preoperative flow assessment were compared.
All patients with first-time isolated CABG in Sweden 2013-2020 were identified in the SWEDEHEART registry (
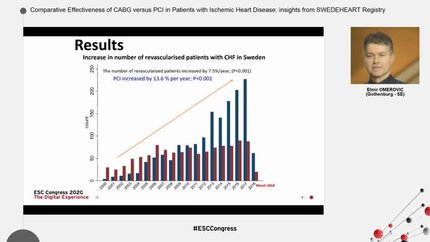
Overall, 2869 patients (15.8%) had flow assessment before surgery, increasing from 7.1% in 2013% to 21.5% in 2020. Patients with flow assessment were younger, had a lower EuroSCORE II, and received fewer distal anastomoses (3.0 ± 0.9 vs 3.2 ± 1,
Preoperative flow assessment was not associated with improved clinical outcomes but with a higher risk for new angiography and new revascularization >2 years after CABG. The results suggest that the use of flow assessment with current cut-off levels may not be applicable in CABG, and further studies are needed.
Contributors

Elmir Omerovic
Author
Dimitrios Venetsanos
Author
Joakim Alfredsson
Author
Andreas Martinsson
Author
Björn Redfors
Author
Amar Taha
Author
Susanne J Nielsen
Author
Anders Jeppsson
Author
You may be interested in