Machine learning modelling using cardiac magnetic resonance images to predict cancer therapy related cardiac dysfunction with external validation in HER2+ breast cancer patients
European Heart Journal Supplements


Abstract
Predicting the risk of cancer therapy-related cardiac dysfunction (CTRCD) remains a challenge. Clinical risk models and conventional cardiac magnetic resonance (CMR) analysis are limited in predicting HER2+ targeted therapy (HER2-TT) CTRCD risk.1 Recent studies suggest that deep learning (DL) applied to medical images can identify phenotypes beyond conventional image interpretation.2
We aimed to determine if DL approaches using CMR cine images pre or early during cancer therapy can predict CTRCD better than clinical risk scores or conventional quantified imaging measures.
Women with early-stage HER2+ breast cancer receiving sequential anthracyclines and trastuzumab from three prospective studies (Toronto: EMBRACE MRI, SPARE-HF and Calgary: CIROC) were included. Patients were seen pre- and post-anthracycline and sequentially during treatment with repeated cardiac imaging (echocardiography and CMR). CTRCD was defined using the Cardiac Review and Evaluation Committee criteria. We calculated the HFA-ICOS risk score, and conventionally measured CMR and echocardiography left ventricular size and function (volumes, ejection fraction, strain). Pre- and post-anthracycline data were used to create various models to predict CTRCD. Multiple machine learning models were used including logistic regression (LR). Deep convolutional neural network architectures were used with CMR short-axis cines at the same timepoints to develop image-based DL models to predict CTRCD. Patients from Toronto were used for model derivation and internal validation, while those from Calgary were used for external validation. To gauge the model performance, we calculated the Area Under the ROC Curve (AUC), sensitivity, specificity and F1 score.
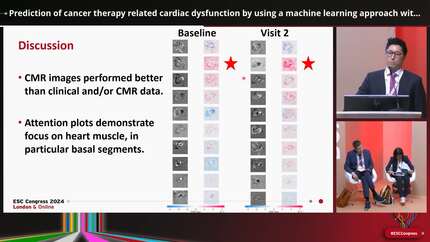
229 patients were included: 176 in the internal (52 CTRCD events; doxorubicin equivalent dose (DED) 211±20mg/m2) and 53 in the external dataset (14 CTRCD events; DED 216±26mg/m2). The mean age was 51.4±9.5 years. Pre-anthracycline LR models (best performing models) for the HFA-ICOS risk score and quantified CMR and echocardiographic parameters demonstrated AUCs of 0.60 (95% CI: 0.57-0.75); 0.69 (0.65-0.73); and 0.78 (0.74-0.81) to discriminate CTRCD, respectively, with F1 scores of 0.21 (0.18-0.25); 0.41 (0.33-0.48); and 0.51 (0.45-0.57) (Figure 1). Baseline CMR short-axis cine DL model demonstrated the highest AUC 0.85 (0.69-0.97) and F1 score 0.69 (0.47-0.86). On external validation, the DL model had an AUC of 0.80 (0.58-0.86) with an F1 score of 0.55 (0.32-0.69), Figure 2. The addition of post-anthracycline clinical data or CMR images did not improve the clinical and DL models’ performance potentially owing to overfitting to less reliable features, Figure 1.
In women with breast cancer receiving anthracyclines and HER2-TT, a DL model using CMR short axis cine images pre-anthracycline had higher discrimination for future CTRCD than clinical and conventional imaging quantification models.
Contributors





You may be interested in