Conduction system versus right ventricular pacing for bradycardia treatment; 1 year outcomes of a prospective, randomized trial in patients with advanced AV disease
EP Europace Journal


Abstract
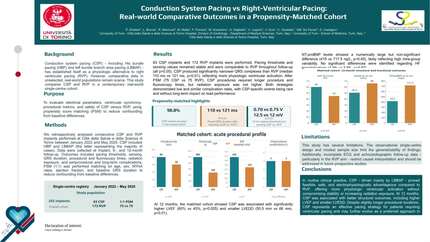
Conduction system pacing (CSP) is a pacing modality that aims to replace right ventricular pacing (RVP) in treating patients with bradycardia. However, there is a lack of data about the differences in outcomes between CSP and RVP.
To compare the effects of CSP vs. RVP on procedural characteristics, left ventricular ejection fraction (LVEF), and composite clinical endpoint in patients with bradycardia and an indication of pacing.
This prospective, multicentre study randomly assigned patients with severe conduction disease to CSP and RVP in a 1:1 ratio between 2021 and 2023. CSP arm patients received either His bundle pacing (HBP) or LBBAP; in the RVP arm, the RV septal lead placement was recommended. Patients are being clinically followed for 3 years after the implantation, and this is a pre-specified analysis of the data after one year of follow-up. Relevant data were collected during the initial hospitalization and one-year follow-up visit and captured in an electronic case report form. The primary endpoint was a change of the LVEF calculated by a Simpson method. The composite clinical endpoint was a combination of cardiovascular death, CRT upgrade, or hospitalization for heart failure. An independent core lab assessed LVEF, and clinical endpoints were evaluated by an independent clinical committee.
Out of 249 patients, 125 were randomized in the RVP arm and 124 in the CSP arm, with no difference in clinical characteristics between the groups. In the CSP group, ten patients received HBP and 109 LBBAP (in 5 patients, deep septal deployment of the pacing lead was unsuccessful, and they obtained RV pacing). Procedural and sciascopy times were longer in CSP than in the RV arm (70 vs. 42 minutes and 8 vs. 3 minutes, p < 0.001 for both). The absolute pacing threshold was lower in the CSP group than in the RVP group (0.44 V vs. 0.56 V, p < 0.001) at the costs of longer impulse duration (0.53 ms vs. 0.4 ms, p < 0.001). After one year of pacing, both groups had the same pacing burden (97%), and in the intention-to-treat analysis, both groups declined in the LVEF. The RVP group decreased from 61% to 57% and the CSP group from 61% to 58%, p < 0.001 for both; however, the decline in the CSP group was smaller (-2% in CSP vs. -4% in RVP, p = 0.03). A significant drop in the LVEF of ≥ 10% occurred in 17 (15%) patients in the RVP group vs. 6 (5%) in the CSP group; p = 0.01. There was no difference in a composite clinical outcome between the groups; it occurred in 9 patients (7%) in the RVP group vs. four patients (3%) in the CSP group, p = 0.15. There was no difference in the device and lead-related complications between the groups (9 in the RVP group and 2 in the CSP group, p = 0.09).
In patients with bradycardia and severe conduction disease, CSP leads to a smaller LVEF decline than RVP one year of pacing. Both pacing methods have similar rates of clinical endpoints, complications, and pacing parameters.
Contributors

K Curila
Author
P Jurak
Author
P Leinveber
Author
J Kupec
Author
J Mizner
Author
J Vesela
Author
P Stros
Author
O Sussenbek
Author
R Smisek
Author
R Polasek
Author
You may be interested in